Download
1 / 10
100 likes | 189 Views
The bulk of a tooth is formed of dentine, which is sensitive to ternperature change and other stimuli. In the centre of the tooth crown, and down the root to the tooth apex, is a hollow space occupied by the pulp, which is soft tissue containing nerves and vessels. The

E N D
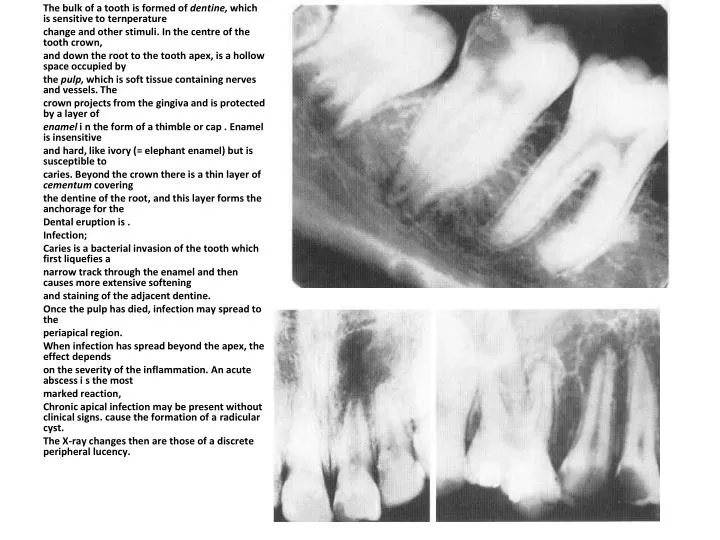
The bulk of a tooth is formed of dentine, which is sensitive to ternperature change and other stimuli. In the centre of the tooth crown, and down the root to the tooth apex, is a hollow space occupied by the pulp, which is soft tissue containing nerves and vessels. The crown projects from the gingiva and is protected by a layer of enamel i n the form of a thimble or cap . Enamel is insensitive and hard, like ivory (= elephant enamel) but is susceptible to caries. Beyond the crown there is a thin layer of cementumcovering the dentine of the root, and this layer forms the anchorage for the Dental eruption is . Infection; Caries is a bacterial invasion of the tooth which first liquefies a narrow track through the enamel and then causes more extensive softening and staining of the adjacent dentine. Once the pulp has died, infection may spread to the periapical region. When infection has spread beyond the apex, the effect depends on the severity of the inflammation. An acute abscess i s the most marked reaction, Chronic apical infection may be present without clinical signs. cause the formation of a radicular cyst. The X-ray changes then are those of a discrete peripheral lucency.
Radiation changes in the jaw Radiation and chemotherapy cause damage to developing teeth. the fetus or infant is irradiated, damage to the developing tooth germ can cause either absence of the tooth or gross hypoplasia, both of primary and secondary dentition. In addition, mandibular growth is retarded and hypoplasia results . Irradiation of the oral tissues (e.g. for soft-tissue sarcoma) affects the salivary glands and the nature of their secretions, which diminish and become more acid. Caries is potentiated in a dry mouth andRadionecrosis Initially, osteoporosis is seen, but the end-stage is a pattern of mixed sclerosis and lysis. Pathological fractures and bone resorption as well as sequestra are seen. Periosteal new bone is not prominent in the mandible.
DDX OF sclerosing lesion of the jaw s; 1-hypercementosis 2-cementoma. 3-post inflammatory sclerosingosteitis. 4-odontomes(complex &compouind). 5-localized fibrous dysplasia. 6-pagets dissease.
generalized dissease effecting teeth&jaws; HypopituitarismHypoplasia of the jaws and teeth and delayed dental age arc found, as would be expected. Hyperparathyroidism Subperiosteal bone resorption is the pathognomonic bony change in this disease. Gigantism Dental separation again results from jaw enlargement, they are difficult teeth to radiograph.
Cyst of jaws; Cysts of the jaws may conveniently be classified into: I. Cysts of denial origin, developmental or post inflammatory 2. Non-dental, developmental or fissural cysts 3. Non-epitheliated cysts .
Post inflammatory Radicular (apical) cysts Most cysts of the jaws are radicular. They lie directly upon the apex of a tooth. which is usually diseased. They follow inflammation of the pulp and apical bone, when a local apical area of chronic inflammation, the granuloma. may result. This is seen radiologically as a poorly defined para-apical area of bone loss rather like a Brodie's abscess. The well-defined radicular cyst results. Its dense opaque margin is continuous with the lamina dura at the periphery of the cyst, but within the cyst the lamina dura is destroyed. These cysts are generally less than 1.5 cnm in diameter and in grossly carious mouths may he multiple . Treatment is by removal of the tooth and curettage. This should result in bony healing with gradual obliteration of the cavity. Should the cyst persist after dental extraction, it is known as a residual cyst and its origin cannot be interred from a radiograph
(i) Odontogenickeratocyst (primordial cyst) These may follow cystic degeneration of the enamel organ before the tooth is formed, so that the cyst replaces the tooth, but they may also arise from cctopicodontogenic epithelium. Should a normal complement of teeth be present, the cyst is assumed to have replaced a supernumerary tooth. Primordial cysts are more common in young men, but may be seen at all ages. They are slow-growing but may reach a very large size and may occupy the entire ascending ramus . The cortex becomes thinned and an axial view also demonstrates expansion in the buccal-lingual plane. They are most commonly seen in the posterior mandible and arc usually monolocular. These cases present either because a critical size is reached and the patient feels a fluctuant swelling of the mandible, or because of secondary infection and purulent discharge. Because of their growth potential, they may abut against an initially unrelated and uneruptcd tooth. A dentigerous cyst is then simulated, although the size and location may help in differentiation. The diagnosis is in any case confirmed by enucleation and histologi cal examination. These cysts are almost inevitably keatinised and are very likely to recur unless removed completely. Long-tern follow-up is therefore advisahle.
(ii) Dentigerous cyst (follicular cyst) Cystic degeneration of the enamel organ may occur after the tooth has been formed but before it has erupted. This results in a cyst related to the crown of an uneruptcd tooth. Cysts enlarge in part because of local hydrostatic imbalance. if the pressure within the cyst exceeds the eruplive pressure of the tooth, that tooth is prevented from erupting. It becomes displaced, often for some distance. Part of the crown always remains in contact with the cyst
2. Developmental (fissural) cysts These presumably occur at sites of fusion of embryonic processes. Such cysts are: a. Medial mandibular. b. Medial rnaxillarvr c. Nasopalatine. The nasopalaline ducts connect the nasal cavity with the palate behind the central incisors. Four ducts are present in utero, two on either side of the midline. Failure of normal ductal obliteration may result in local epithelial remnants undergoing cystic degeneration. d. Globulomaxillar_y. These cysts look like an inverted pear and lie between the upper lateral incisor and canine, the roots of which are diverged. There is some doubt as to whether these are fissural or inflammatory. The majority are odontogenickeratocysts.
Non epithelialised bone cyst; Simple bone cyst. These may follow trauma and are thus also known as traumatic cysts. They appear in young patients, usually boys, in the posterior aspect of the body of the mandible. Like other types of cyst, they are vaguely spherical, well-defined, and surrounded by a thin dense zone of reactive sclerosis. Aneurysrnal bone cyst. These present as a well-defined expansile radiolucency, displacing teeth. Again, the lesion is not common i n the jaws. and histology is usually needed to confirm its identity. They may be secondary to other tumours