Download
1 / 1
10 likes | 122 Views
Introduction. Results: CP vs. AP. Methods. Conclusions. F ully Automated IMRT T reatment P lanning is Feasible for H&N C ancer: A Prospective Study using Overlap V olume H istogram (OVH) S trategy.

E N D
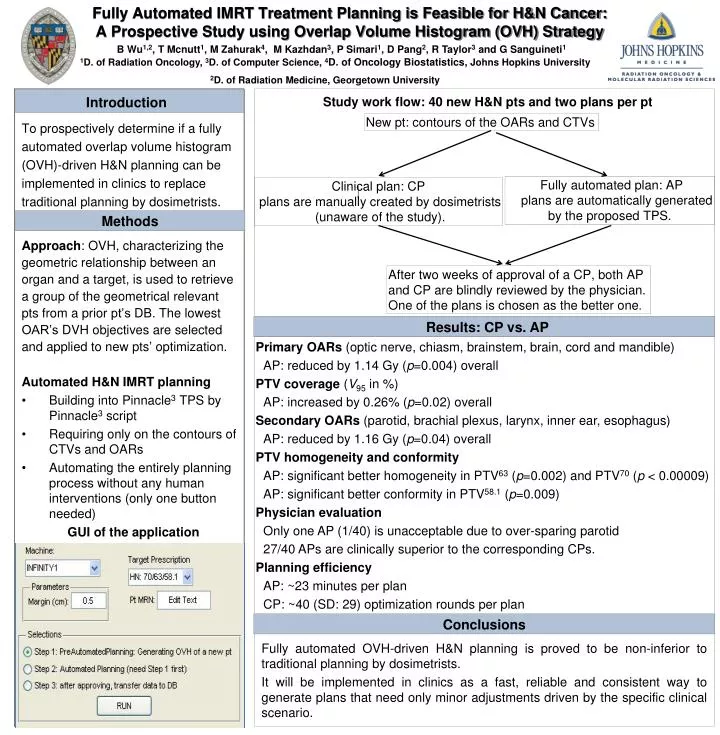
Introduction Results: CP vs. AP Methods Conclusions Fully Automated IMRT Treatment Planning is Feasible for H&N Cancer: A Prospective Study using Overlap Volume Histogram (OVH) Strategy B Wu1,2, T Mcnutt1, M Zahurak4, M Kazhdan3, P Simari1, D Pang2, R Taylor3 and G Sanguineti1 1D. of Radiation Oncology, 3D. of Computer Science, 4D. of Oncology Biostatistics, Johns Hopkins University 2D. of Radiation Medicine, Georgetown University Study work flow: 40 new H&N pts and two plans per pt New pt: contours of the OARs and CTVs To prospectively determine if a fully automated overlap volume histogram (OVH)-driven H&N planning can be implemented in clinics to replace traditional planning by dosimetrists. Approach: OVH, characterizing the geometric relationship between an organ and a target, is used to retrieve a group of the geometrical relevant ptsfrom a prior pt’s DB. The lowest OAR’s DVH objectives are selected and applied to new pts’ optimization. Automated H&N IMRT planning • Building into Pinnacle3 TPS by Pinnacle3script • Requiring only on the contours of CTVs and OARs • Automating the entirely planning process without any human interventions (only one button needed) GUI of the application Fully automated OVH-driven H&N planning is proved to be non-inferior to traditional planning by dosimetrists. It will be implemented in clinics as a fast, reliable and consistent way to generate plans that need only minor adjustments driven by the specific clinical scenario. Fully automated plan: AP plans are automatically generated by the proposed TPS. Clinical plan: CP plans are manually created by dosimetrists (unaware of the study). After two weeks of approval of a CP, both AP and CP are blindly reviewed by the physician. One of the plans is chosen as the better one. • Primary OARs (optic nerve, chiasm, brainstem, brain, cord and mandible) • AP: reduced by 1.14 Gy (p=0.004) overall • PTV coverage (V95 in %) • AP: increased by 0.26% (p=0.02) overall • Secondary OARs (parotid, brachial plexus, larynx, inner ear, esophagus) • AP: reduced by 1.16 Gy (p=0.04) overall • PTV homogeneity and conformity • AP: significant better homogeneity in PTV63 (p=0.002) and PTV70 (p < 0.00009) • AP: significant better conformity in PTV58.1 (p=0.009) • Physician evaluation • Only one AP (1/40) is unacceptable due to over-sparing parotid • 27/40 APs are clinically superior to the corresponding CPs. • Planning efficiency • AP: ~23 minutes per plan • CP: ~40 (SD: 29) optimization rounds per plan