Download
1 / 45
450 likes | 647 Views
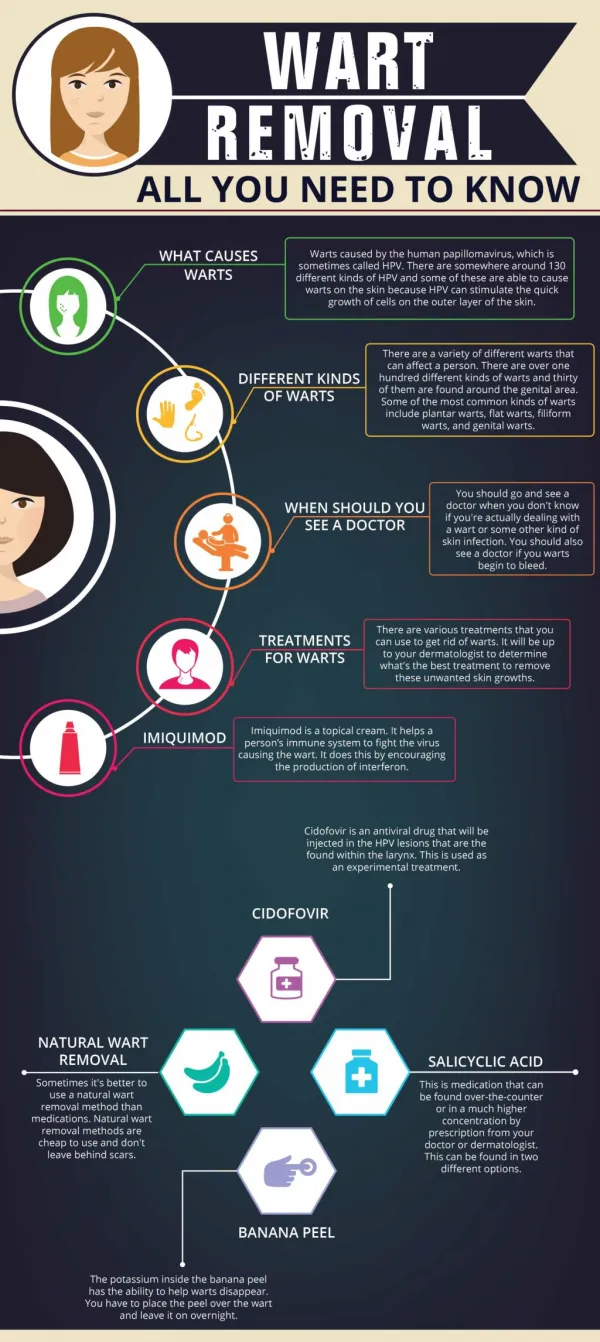
Warts. Medical Student Core Curriculum in Dermatology. Last updated July 29, 2011. Module Instructions.

E N D
Warts Medical Student Core Curriculum in Dermatology Last updated July 29, 2011
Module Instructions • The following module contains a number of blue, underlined terms which are hyperlinked to the dermatology glossary, an illustrated interactive guide to clinical dermatology and dermatopathology. • We encourage the learner to read all the hyperlinked information.
Goals and Objectives • The purpose of this module is to help medical students develop a clinical approach to the evaluation and initial management of patients presenting with warts. • By completing this module, the learner will be able to: • Identify and describe the morphology of various types of warts • Discuss the pathogenesis of warts • Develop an initial treatment plan for a patient with warts • Describe the technique of cryotherapy • List the side effects of cryotherapy
Case One Megan Driskell
Case One: History • HPI: Megan is an 8-year-old girl who presents to her pediatrician’s office with bumps on her fingers and hands. They have been present for 3 months without change and are asymptomatic. • PMH: no chronic illnesses or prior hospitalizations • Allergies: no known allergies • Medications: none • Family history: no affected family members • Social history: lives at home with parents and attends school • ROS: negative
Case One: Question 1 • How would you describe these lesions? • Hyperkeratotic and umbilicated papules and nodules • Hyperkeratotic, endophytic papules and nodules • Hyperkeratotic, exophytic papules and nodules • Smooth and umbilicated papules and nodules • Smooth, exophytic papules and nodules
Case One: Question 1 Answer: c • How would you describe these lesions? • Hyperkeratotic and umbilicated papules and nodules (these papules are not umbilicated) • Hyperkeratotic, endophytic papules and nodules (these papules are growing outward, not inward) • Hyperkeratotic, exophytic papules and nodules • Smooth and umbilicated (marked by a depressed spot) papules and nodules (more characteristic of molluscum contagiosum) • Smooth, exophytic papules and nodules (these papules are not smooth)
Hyperkeratotic, exophytic (growing outward), dome-shaped papules or nodules Most common on fingers, dorsal hands, knees or elbows but may occur anywhere Punctate black dots representing thrombosed capillaries May koebnerize – spread with skin trauma Clinical Features of Verruca Vulgaris
Epidemiology • One of the top three skin problems in children • Cutaneous warts occur in 20% of school-aged children; also commonly found in young adults • Males and females are equally affected
Case One: Question 2 • Verruca vulgaris is caused by: • Human immunodeficiency virus • Human papillomavirus • Pox virus • Herpes virus • Varicella-zoster virus
Case One: Question 2 Answer: b • Verruca vulgaris is caused by: • Human immunodeficiency virus • Human papillomavirus • Pox virus • Herpes virus • Varicella-zoster virus
Human Papillomavirus (HPV): Overview Warts are caused by HPV HPV infects skin and mucosal epithelia HPV causes a variety of wart morphologies Verruca vulgaris: common warts Verrucae planae: flat warts Palmoplantar warts Condylomataacuminata: external genital warts The type of HPV determines the wart morphology 13
Role of HPV in Cutaneous Disease • HPV can be transmitted by skin-to-skin contact or through contaminated surfaces or objects • Patients can also spread virus from lesion to unaffected skin • HPV infects the basal keratinocytes of cutaneous and mucosal epithelium
Clinical Features of Verrucae Planae: Flat Warts • Skin-colored or pink • Smooth-surfaced, slightly elevated, flat-topped papules • Dorsal hands, arms, face (exposed surfaces)
Clinical Features of Palmoplantar Verruca • Thick, endophytic papules • Central depression • Plantar warts may be painful when walking • Mosaic warts: plantar warts coalescing into large plaques
General Treatment Principles • Majority of all warts will spontaneously resolve in 1-2 years without scar • Therefore important to choose a therapy with low toxicity and low risk of scarring • No specific antiviral therapy for cure • Most treatments are destructive or aim at stimulating the immune response to HPV • Recurrence rates are high
Common Wart Treatment Options • Watchful waiting – majority of all warts will spontaneously resolve in 1-2 years without scarring • Cryotherapy – liquid nitrogen (see following slide for more information) • Salicylic acid – with occlusion and removal of the dead skin (filing, pumice stone) • For patients who do not respond to the above therapies, refer to a dermatologist
Cryotherapy • Click here for an instructional video on cryotherapy • Side effects of cryotherapy include: • PIPA (post-inflammatory pigment alteration) • In individuals with darker skin types, more likely to cause hypopigmentation (see pre and post-cryo photos below) • Scar • Pain • Blister • Nail dystrophy
Side Effects of Cryotherapy Post inflammatory hyperpigmentation Wart ring post cryotherapy
Flat Wart Treatment Options • Common 1st line tx: • Cryotherapy • Salicylic acid (caution using on face) • Topical tretinoin
Palmoplantar Wart Treatment Options • 1st line treatment is the same as common wart therapy (often requires stronger dosing, e.g. 40% salicylic acid vs. 17% salicylic acid) • Referral to a dermatologist may be made for chemotherapeutic agents (e.g. topical 5-Fluorouracil)
Case Two Jonathan Cohen
Case Two: History • HPI: Mr. Cohen is a 21-year-old man who comes into the STD clinic because of an increasing number of bumps on his penis over the last year. • PMH: no chronic illnesses or prior hospitalizations • Allergies: no known allergies • Medications: none • Family history: noncontributory • Social history: studying economics at a nearby university • ROS: negative
Case Two: Question 1 • How would you describe these lesions? • Pearly, vesicular papules • Smooth, indurated plaques • Verrucous exophytic papules • Waxy, stuck-on plaques
Case Two: Question 1 Answer: c How would you describe these lesions? Pearly, vesicular papules Smooth, indurated plaques Verrucous exophytic papules Waxy, stuck-on plaques
Clinical Features of external genital warts • Sessile, exophytic papules • May be broad-based papules or large confluent plaques • External genitalia, perineum, perianal, inguinal fold, mons pubis
Comparison of molluscum and genital warts Molluscum Contagiosum (smooth, dome-shaped papules with central umbilication) External Genital Warts (hyperkeratotic, exophytic papules and plaques)
Case Two: Question 2 • What further elements in the patient’s history would you need to complete your evaluation? • Medications • Sexual history • Surgical history • Allergies
Case Two: Question 2 Answer: b • What further elements in the patient’s history would you need to complete your evaluation? • Medications • Sexual history • Surgical history • Allergies 31
HPV Infection Genital infection with HPV is transmitted by sexual contact from partners with clinical or subclinical infection
External Genital Warts (EGW) • HPV infection is one of the most common STIs • Risk factors: sexual intercourse at an early age, numerous partners, unprotected exposure • Patients should receive counseling about condom usage, STI prevention, and potential STI testing for sexual partners • Effective prophylactic HPV vaccine is available for prevention of genital warts • Immunosuppression from HIV infection, organ transplant, etc. can lead to: • Increased frequency of HPV infection • Persistent infection • More difficulties in treatment
Case Two: Question 3 • What is the most likely HPV type leading to this patient’s disease? • 2 • 6 • 16 • 31 • 34
Case Two: Question 3 Answer: b • What is the most likely HPV type leading to this patient’s disease? • 2 • 6 • 16 • 31 • 34
Case Two: Question 4 • Which of the following treatments could you use for external genital warts? • Cryotherapy • Imiquimod • Salicylic acid • All of the above
Case Two: Question 4 Answer: d • Which of the following treatments could you use for external genital warts? • Cryotherapy (liquid nitrogen is used to freeze the tissue at the cellular level) • Imiquimod (a cream of this interferon inducer can be applied 3x per week, response takes up to 12 weeks) • Salicylic acid (this beta hydroxy acid is applied, occluded for 5-6 days, the wart is pared down, and then the cycle is repeated) • All of the above
Treatment (cont.) • Other destructive methods can be used as well to treat EGW • Laser • Electrocautery and curettage • Surgical debulking • Always use protective mask
Imiquimod: True or False • Imiquimod therapy is an off label use for treatment of external genital warts. • True • False
Imiquimod: True or False False • Imiquimod is FDA approved for treatment of EGW • Interacts with Toll-like receptors 7 and 8 to increase cytokines from macrophages • Clearance of 50% EGW compared to placebo of 11% • A disadvantage to this treatment is cost
Prevention Reminder: HPV Vaccine • Two HPV vaccines are licensed by the FDA and recommended by the CDC • Gardasil™ and Cervarix™ • Both vaccines are effective against HPV types 16 and 18, which cause most cervical cancers • Gardasil is also effective against HPV types 6 and 11, which cause most genital warts in females and males • 100% protection in prevention of genital warts during 5-year follow up period studied
Take Home Points • Warts are caused by human papilloma viruses • Numerous morphologies exist: common, flat, palmoplantar, external genital • Treatment is difficult and there are many options available • A vaccine of certain HPV types has proven effective in reducing external genital warts
Acknowledgements • This module was developed by the American Academy of Dermatology Medical Student Core Curriculum Workgroup from 2008-2012. • Primary authors: Kari L. Martin, MD; Susan K. Ailor, MD, FAAD. • Peer reviewers: Renee M. Howard, MD, FAAD; Erin F. D. Mathes, MD, FAAD, FAAP, Timothy G. Berger, MD, FAAD. • Revisions and editing: Sarah D. Cipriano, MD, MPH; Meghan Mullen Dickman. Last revised July 2011.
References • Berger T, Hong J, Saeed S, Colaco S, Tsang M, Kasper R. The Web-Based Illustrated Clinical Dermatology Glossary. MedEdPORTAL; 2007. Available from: www.mededportal.org/publication/462. • Gibbs S, Harvey I. “Topical treatments for cutaneous warts.” Cochrane Rev. Vol 1. 2009. Online at eMedicine:http://emedicine.medscape.com/article/1131981-overview. Updated 12/2009. • Kirnbauer R, Lenz P, Okun MM. “Chapter 78. Human Papillomavirus” (chapter). Bolognia JL, Jorizzo JL, Rapini R: Dermatology. 2nd ed. Mosby Elsevier; 2008. 1183-1198. • Silverberg NB. “Human papillomavirus infections in children.” Current Opinion in Pediatrics. 16:402-409. 2004.