Download
1 / 1
10 likes | 111 Views
Testing End-of-Life Decision Making by Proxy – Using Conjoint Analysis for those with Intellectual Disability Kathleen Fisher, PhD CRNP; Fredrick K. Orkin ; MD, MBA, MSc; Michael J. Green, MD, MS Drexel University, Philadelphia, PA USA. Introduction and Background . Results .

E N D
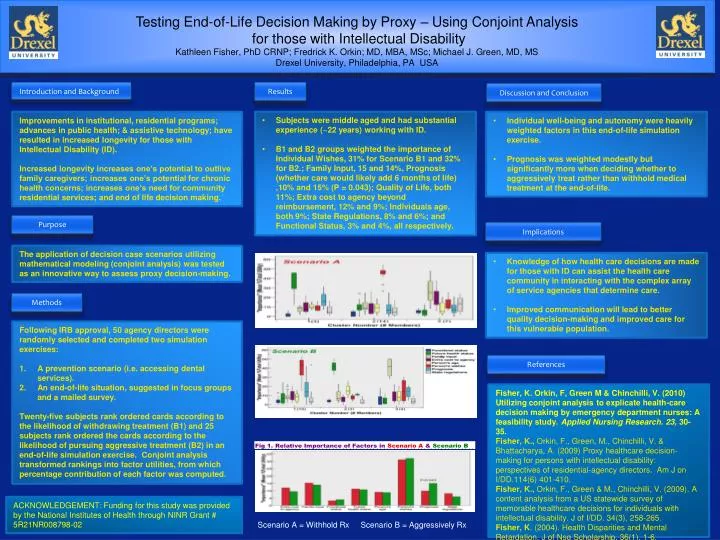
Testing End-of-Life Decision Making by Proxy – Using Conjoint Analysis for those with Intellectual Disability Kathleen Fisher, PhD CRNP; Fredrick K. Orkin; MD, MBA, MSc; Michael J. Green, MD, MS Drexel University, Philadelphia, PA USA Introduction and Background Results Discussion and Conclusion Improvements in institutional, residential programs; advances in public health; & assistive technology; have resulted in increased longevity for those with Intellectual Disability (ID). Increased longevity increases one’s potential to outlive family caregivers; increases one’s potential for chronic health concerns; increases one’s need for community residential services; and end of life decision making. • Subjects were middle aged and had substantial experience (~22 years) working with ID. • B1 and B2 groups weighted the importance of Individual Wishes, 31% for Scenario B1 and 32% for B2.; Family Input, 15 and 14%, Prognosis (whether care would likely add 6 months of life) ,10% and 15% (P = 0.043); Quality of Life, both 11%; Extra cost to agency beyond reimbursement, 12% and 9%; Individuals age, both 9%; State Regulations, 8% and 6%; and Functional Status, 3% and 4%, all respectively. • Individual well-being and autonomy were heavily weighted factors in this end-of-life simulation exercise. • Prognosis was weighted modestly but significantly more when deciding whether to aggressively treat rather than withhold medical treatment at the end-of-life. Purpose Implications The application of decision case scenarios utilizing mathematical modeling (conjoint analysis) was tested as an innovative way to assess proxy decision-making. • Knowledge of how health care decisions are made for those with ID can assist the health care community in interacting with the complex array of service agencies that determine care. • Improved communication will lead to better quality decision-making and improved care for this vulnerable population. Methods • Following IRB approval, 50 agency directors were randomly selected and completed two simulation exercises: • A prevention scenario (i.e. accessing dental services). • An end-of-life situation, suggested in focus groups and a mailed survey. • Twenty-five subjects rank ordered cards according to the likelihood of withdrawing treatment (B1) and 25 subjects rank ordered the cards according to the likelihood of pursuing aggressive treatment (B2) in an end-of-life simulation exercise. Conjoint analysis transformed rankings into factor utilities, from which percentage contribution of each factor was computed. References Fisher, K. Orkin, F, Green M & Chinchilli, V. (2010) Utilizing conjoint analysis to explicate health-care decision making by emergency department nurses: A feasibility study. Applied Nursing Research. 23, 30-35. Fisher, K., Orkin, F., Green, M., Chinchilli, V. & Bhattacharya, A. (2009) Proxy healthcare decision-making for persons with intellectual disability: perspectives of residential-agency directors. Am J on I/DD.114(6) 401-410. Fisher, K., Orkin, F., Green & M., Chinchilli, V. (2009). A content analysis from a US statewide survey of memorable healthcare decisions for individuals with intellectual disability. J of I/DD. 34(3), 258-265. Fisher, K. (2004). Health Disparities and Mental Retardation. J of Nsg Scholarship, 36(1), 1-6. ACKNOWLEDGEMENT: Funding for this study was provided by the National Institutes of Health through NINR Grant # 5R21NR008798-02 Scenario A = Withhold Rx Scenario B = Aggressively Rx