Download

1 / 17
180 likes | 644 Views
Sacroiliac Joint. J. Scott Bainbridge, MD www.DenverBackPainSpecialists.com. SIJ Background. Proposed as potential source of pain by Goldthwaite in 1905 Incidence of SIJ pain in LBP population: 18-40% (Schwarzer, Maigne, DePalma, Liliang, Schofferman). SIJ Anatomy. SIJ Anatomy.

E N D
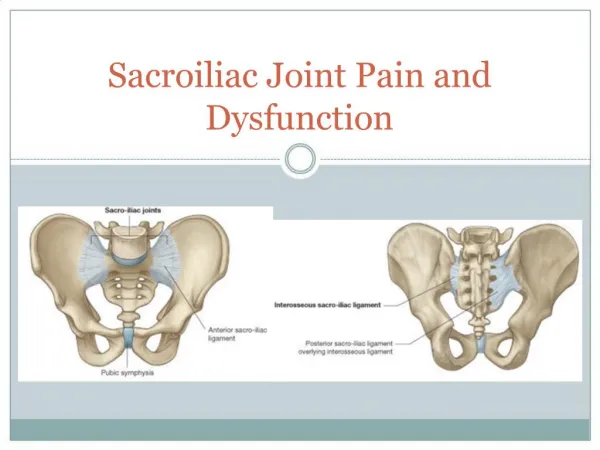
Sacroiliac Joint J. Scott Bainbridge, MD www.DenverBackPainSpecialists.com
SIJ Background • Proposed as potential source of pain by Goldthwaite in 1905 • Incidence of SIJ pain in LBP population: 18-40% (Schwarzer, Maigne, DePalma, Liliang, Schofferman)
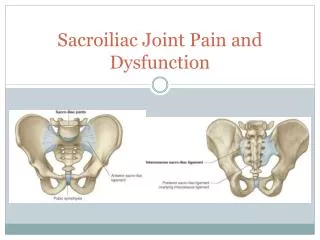
SIJ Anatomy • Diarthrodial joint • Hyalin cartilage, fibrocartilage also on ilial side • Interlocking contours • Ligaments: anterior and posterior SIL, interosseous SIL, sacrospinous and sacrotuberous • Muscles: paraspinous, gluteal, psoas, iliacus, abdominal, sartorius, rectus femoris, hamstrings, latissimus dorsi (lumbodorsal fascia) • Nutation
SIJ Innervation • Early: Cunningham’s…, Bernard and Cassidy, Ikeda, Nagakawa, etc. included anterior innervation (ventral rami) • Fortin et al, Grob et al: macroscopic and fetal microscopic fetal studies: innervation entirely dorsal rami (S1-3[4]) • Yin, Willard, Carreiro, Dreyfuss: defined (fluoro) course of sacral dorsal rami; reported SIJRF pilot technique and results
S-1 Dorsal Rami Yin, et al. Spine 2003
Diagnosis • X-ray, MRI, CT, bone scan generally not helpful except to rule in/out fracture, stress response, infection, tumor, sacroiliitis • Arthrogram may show capsular disruption • Need double intraarticular SIJ blocks to diagnose, although single IA, posterior ligament, or dorsal rami blocks have been used by various authors/practitioners • Blockade of the L5 Dorsal Rami and Sacral 1-3 lateral branches, using the multi-site, multi-depth technique of Dreyfuss, et al. (Pain Medicine 2009) is necessary for radiofrequency neurotomy (RFN) screening.
Diagnosis - History • Unilateral pain at or below PSIS, PSIS pointing (Fortin, Maigne) • , no pain above L5, pain over SIJ and Buttock (Dreyfuss, et al)
Diagnosis – Physical Exam • Maigne: Patrick’s – trend – p=0.9 • Broadhurst and Bond: double blind, lido v saline • FABER (Flexion, ABduction, External Rotation) • POSH (POsterior SHear) • REAB (REsisted ABduction) • 100% specificity, 77-80% specificity @ 70% < pain
Diagnosis – Physical Exam • Dreyfuss, et al (multidisciplinary expert panel) • 12 key pain, Hx, and PE parameters • Single block, 90% relief • PSIS pointing, no pain above L5, sacral sulcus tenderness, pain over SIJ/buttock • Gillet’s test best of provocative maneuvers
Diagnosis – Physical Exam • Van der Wurff, et al, 2006 • Double blocks, >50% relief • 3 of 5 positive tests (distraction, compression, thigh thrust, Patrick, Gaenslen) • Sensitivity .85, specificity .79 • PPV .77, NPV .87
Discogenic: Centralization w McKenzie method • Pain w rising from sitting • Sacroiliac: Unilateral pain; No lumbar pain • Pain rising from sitting • 3/5 provocation tests: distraction, compression, sacral thrust, thigh thrust, Gaenslen’s • LZJ: no pain rising from sitting
SIJ - Treatment • Manual therapy • Exercise (m. balance, stabilization) • Medication • IA injection (corticosteroids) • Prolotherapy • PRP – Platelet Rich Plasma • Neuromodulation • Dennervation (RF neurotomy)