Download
1 / 21
240 likes | 312 Views
Learn about chickenpox and herpes zoster, their clinical features, complications, diagnosis, treatment, prevention, and control strategies. Understand the importance of immunization and general measures to manage outbreaks effectively.

E N D
Introduction • Chickenpox: Acute, highly contagious which occurs mostly in children • Herpes zoster: Affects mostly the elderly and immunocompromisedpersons.
chickenpox • Benign disease • It extracts a high price in terms of absenteeism from school, parental leave and medical costs
Agent • Double - stranded DNA virus • Herpesviridae family (human α herpes virus 3) • Only one serotype is known.
Host • Primarily a disease of childhood • 90% of cases occur before 13 years of age • Natural infection confers lifelong immunity • Latent in sensory root ganglia • Mortality rates in children < 2 per 100,000. • Mortality risk for adults is 15 times higher
Environment • Seasonal variation with peak incidence in winter and spring
Transmission • Source of infection case of chickenpox as subclinical cases are rare • Direct contact or air borne spread of • Infected droplets or droplet nuclei. • SAR over 90%
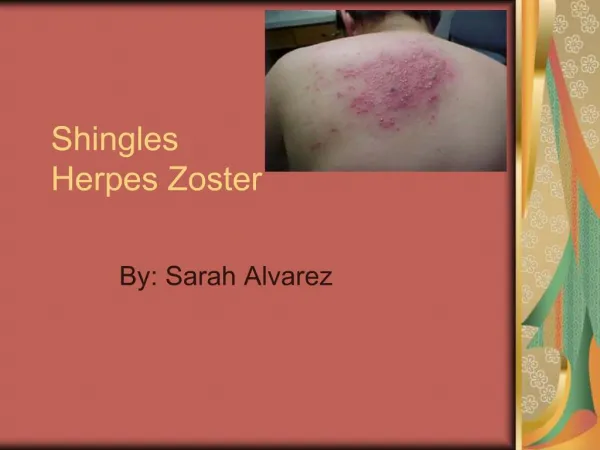
Clinical Features • IP: 13 to 17 days. • Pre eruptive stage: fever, malaise and shivering. (1-2 days) • The rash • Centrifugally. • Maculo - papules, vesicles, and scabs • Rapid evolution and pleomorphism. • Appears in crops with each exacerbation of fever • Healing within 4 - 5 days and the crusts fall within 1-2 weeks
Complications • Secondary bacterial infection • Meningo encephalitis and reye’s: aspirin during acute phase • Congenital varicella syndrome: cicatricial skin scarring, hypoplasia of extremity, mental retardation and LBW
Diagnosis • History of exposure and clinical features • Tzanck smear of vesicular fluid: mltinucleated giant and epithelial cells with eosinophilicintranuclear inclusion bodies • Electron microscopy or PCR • Direct fluorescent antibody (DFA) tests
Herpes Zoster • 10% and 20% of cases of chicken pox develop by herpes zoster later in life • Vesicular eruptions, typically unilateral and follow a dermatomal distribution • Most commonly involved are thoracic and lumbar • >50yrs, HIV & advanced malignancies • Permanent neuro damage
Treatment • No specific treatment for uncomplicated • Acyclovir for complicated • Herpes zoster: Acyclovir and famciclovir
Prevention and Control • Active Immunization • Passive Immunization • General measures
Active Immunization • Live attenuated vaccine • The OKA strain • A single dose achieves over 95% seroconversion • After one year of age • For 1-13 years: 0.5 ml SC single dose • > 13 years of age two doses @ 4 - 8 weeks apart. • Side effects are rare.
Active Immunization: WHO Position • Other vaccine preventable diseases cause greater morbidity and mortality • Varicella vaccine is not a high priority • Considered in countries where this • Disease is a relatively important public health and where the vaccine is affordable, and where high (85% - 90%) and sustained vaccine coverage can be achieved
Passive Immunization • Zoster immune globulin (VZIG) • HRG: immunocompromised, susceptible pregnant women, and new born infants. • Administered as soon as possible after Exposure (within 96 h) at the dose of 125 IU per 10 kg body weight IM injection.
General measures • Cases need to be isolated till all the lesions have crusted (six days) • Concurrent disinfection of articles soiled from discharges from the nose, throat, and from lesions • Outbreaks of chickenpox must be notified.