Download
1 / 1
10 likes | 252 Views
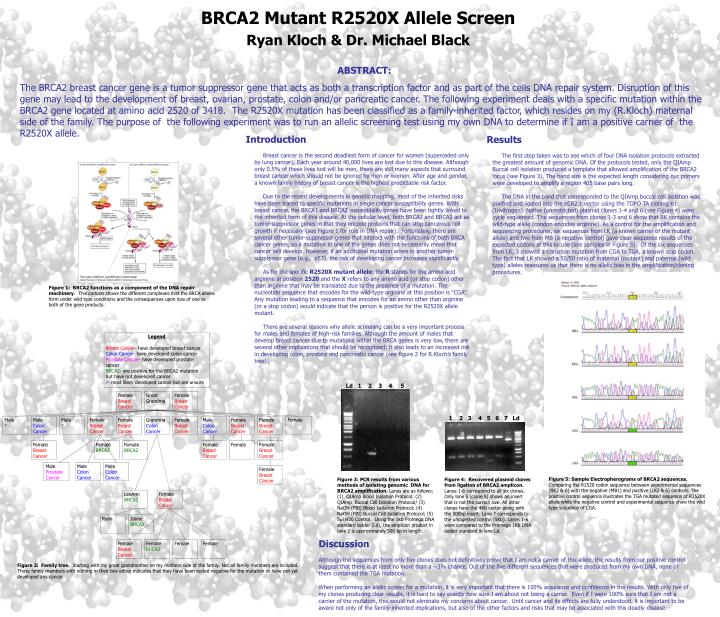
Female Breast Cancer. Great Grandma. Female Breast Cancer. Male Colon Cancer. Male ?. Female Breast Cancer. Female Breast Cancer. Grandma Colon Cancer. Female Breast Cancer. Male Colon Cancer. Female Breast Cancer. Female Breast Cancer. Female. Female Breast Cancer.

E N D
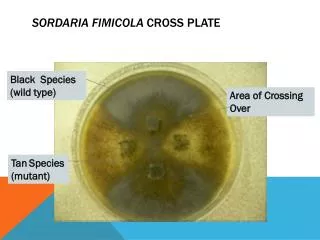
Female Breast Cancer Great Grandma Female Breast Cancer Male Colon Cancer Male ? Female Breast Cancer Female Breast Cancer Grandma Colon Cancer Female Breast Cancer Male Colon Cancer Female Breast Cancer Female Breast Cancer Female Female Breast Cancer Female BRCA2 Female BRCA2 Female Breast Cancer Female Female Breast Cancer Male Prostate Cancer Male Colon Cancer Male Colon Cancer Female Breast Cancer LeeAnn BRCA2 Female Breast Cancer Ryan Jaime BRCA2 Female Breast Cancer Female BRCA2 Female Female Legend Breast Cancer- have developed breast cancer Colon Cancer- have developed colon cancer Prostate Cancer- have developed prostate cancer BRCA2- are positive for the BRCA2 mutation but have not developed cancer ?- most likely developed cancer but are unsure Male ? Figure 2: Family tree. Starting with my great grandmother on my mothers side of the family. Not all family members are included. Those family members with nothing in their box either indicates that they have been tested negative for the mutation or have not yet developed any cancer. BRCA2 Mutant R2520X Allele Screen Ryan Kloch & Dr. Michael Black ABSTRACT: The BRCA2 breast cancer gene is a tumor suppressor gene that acts as both a transcription factor and as part of the cells DNA repair system. Disruption of this gene may lead to the development of breast, ovarian, prostate, colon and/or pancreatic cancer. The following experiment deals with a specific mutation within the BRCA2 gene located at amino acid 2520 of 3418. The R2520X mutation has been classified as a family-inherited factor, which resides on my (R.Kloch) maternal side of the family. The purpose of the following experiment was to run an allelic screening test using my own DNA to determine if I am a positive carrier of the R2520X allele. • Introduction • Breast cancer is the second deadliest form of cancer for women (superceded only by lung cancer). Each year around 40,000 lives are lost due to this disease. Although only 0.5% of these lives lost will be men, there are still many aspects that surround breast cancer which should not be ignored by men or women. After age and gender, a known family history of breast cancer is the highest predictable risk factor. • Due to the recent developments in genetic mapping, most of the inherited risks have been traced to specific mutations in single cancer susceptibility genes. With breast cancer, the BRCA1 and BRCA2 susceptibility genes have been tightly linked to the inherited form of this disease. At the cellular level, both BRCA1 and BRCA2 act as tumor-suppressor genes in that they encode proteins that can stop cancerous cell growth if necessary (see Figure 1 for role in DNA repair). Fortunately, there are several other tumor-suppressor genes that interact with the functions of both BRCA cancer genes, so a mutation in one of the genes does not necessarily mean that cancer will develop. However, if an additional mutation arises in another tumor-suppressor gene (e.g., p53), the risk of developing cancer increases significantly. • As for the specific R2520X mutant allele: the R stands for the amino acid arginine at position 2520 and the X refers to any amino acid (or stop codon) other than arginine that may be translated due to the presence of a mutation. The nucleotide sequence that encodes for the wild-type arginine at this position is “CGA”. Any mutation leading to a sequence that encodes for an amino other than arginine (or a stop codon) would indicate that the person is positive for the R2520X allele mutant. • There are several reasons why allelic screening can be a very important process for males and females of high-risk families. Although the amount of males that develop breast cancer due to mutations within the BRCA genes is very low, there are several other implications that should be recognized: it also leads to an increased risk in developing colon, prostate and pancreatic cancer (see figure 2 for R.Kloch’s family tree). • Results • The first step taken was to see which of four DNA isolation protocols extracted the greatest amount of genomic DNA. Of the protocols tested, only the QIAmp Buccal cell isolation produced a template that allowed amplification of the BRCA2 locus (see Figure 3). The band size is the expected length considering our primers were developed to amplify a region 405 base pairs long. • The DNA in the band that corresponded to the QIAmp buccal cell isolation was purified and ligated into the pCR2.1 vector using the TOPO TA cloning kit (Invitrogen). Native (unrestricted) plasmid clones 1-4 and 6 (see Figure 4) were cycle sequenced. The sequences from clones 1-3 and 6 show that RK contains the wild-type allele (condon encodes arginine). As a control for the amplification and sequencing procedures, six sequences from LK (a known carrier of the mutant allele) and two from MB (a negative control) gave clear sequence results of the expected codons at this locuse (see samples in Figure 5). Of the six sequences from LK, 3 showed a transition mutation from CGA to TGA, a known stop codon. The fact that LK showed a 50/50 ratio of maternal (mutant) and paternal (wild type) alleles reassures us that there is no allelic bias in the amplification/cloning procedures. Figure 1: BRCA2 functions as a component of the DNA repair machinery. This cartoon shows the different complexes that the BRCA alleles form under wild type conditions and the consequences upon loss of one or both of the gene products. Ld 1 2 3 4 5 1 2 3 4 5 6 7 Ld Figure 5: Sample Electropherograms of BRCA2 sequences. Comparing the R2520 codon sequence between experimental sequences (RK2 & 6) with the negative (MB1) and positive (LK2 & 6) controls. The positive control sequence illustrates the TGA mutated sequence of R2520X allele while the negative control and experimental sequence show the wild type sequence of CGA. • Figure 3: PCR results from various methods of isolating genomic DNA for BRCA2 amplification. Lanes are as follows: (1) QIAmp Blood Isolation Protocol; (2) QIAmp Buccal Cell Isolation Protocol/ (3) NaOH (FBI) Blood Isolation Protocol; (4) NaOH (FBI) Buccal Cell Isolation Protocol; (5) 5l H20 Control. Using the 1kb Promega DNA standard ladder (Ld), the amplicon product in lane 2 is approximately 500 bp in length. Figure 4: Recovered plasmid clones from ligation of BRCA2 amplicon. Lanes 1-6 correspond to all six clones. Only lane 5 (clone 5) shows an insert that is not the correct size. All other clones have the 4Kb vector along with the 500bp insert. Lane 7 corresponds to the undigested control (5Kb). Lanes 1-6 were compared to the Promega 1Kb DNA ladder standard in lane Ld. Discussion Although the sequences from only five clones does not definitively prove that I am not a carrier of this allele, the results from our positive control suggest that there is at least no more than a ~3% chance. Out of the five different sequences that were produced from my own DNA, none of them contained the TGA mutation. When performing an allelic screen for a mutation, it is very important that there is 100% assurance and confidence in the results. With only five of my clones producing clear results, it is hard to say exactly how sure I am about not being a carrier. Even if I were 100% sure that I am not a carrier of the mutation, this would not eliminate my concerns about cancer. Until cancer and its effects are fully understood, it is important to be aware not only of the family-inherited implications, but also of the other factors and risks that may be associated with this deadly disease.