Download

1 / 1
10 likes | 120 Views
REMOTE SYNCHRONOUS REVASCULARISATION TECHNIQUE FOR ABDOMINAL WALL TRANSPLANTATION: THE OXFORD EXPERIENCE Georgios Vrakas, Henk Giele , Srikanth Reddy, Sanjay Sinha, Peter Friend, Anil Vaidya Oxford Transplant Centre. 2402152. Replace with logo. Objectives. Results.

E N D
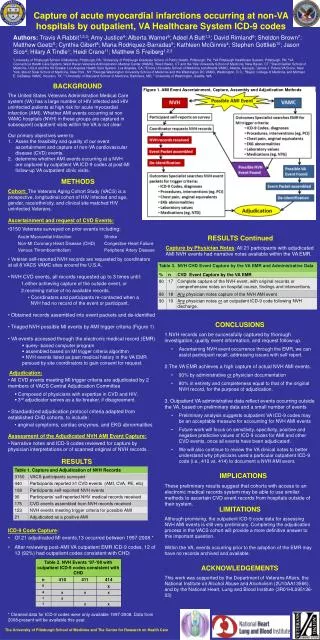
REMOTE SYNCHRONOUS REVASCULARISATION TECHNIQUE FOR ABDOMINAL WALL TRANSPLANTATION: THE OXFORD EXPERIENCE Georgios Vrakas, HenkGiele, Srikanth Reddy, Sanjay Sinha, Peter Friend, Anil Vaidya Oxford Transplant Centre 2402152 Replace with logo Objectives Results Between April 2012 and May 2013, 6 patients underwent small bowel transplantation and synchronous remote revascularisation of their abdominal wall grafts. Mean cold ischaemia time (CIT) for the abdominal wall graft was 338 minutes (range 320-360 minutes). Mean primary warm ischaemia time (PWIT) was 46 minutes (range 43- 55 minutes). Mean secondary warm ischemia time (SWIT) was 73 minutes (range 62- 86 minutes) In 5 cases the abdominal wall graft was inset orthotopically on the recipient’s inferior epigastric vessels at the end of the visceral transplant. In one case the recipient’s IE had poor flow and therefore the graft was reconnected to the ulnar artery. Subsequently a saphenous loop graft from the internal mammary artery (IMA) was used for vascularisation 6 weeks later. One patient died from uncontrolled sepsis 12 weeks after the transplant with a functioning abdominal wall graft. All 6 recipients preserved function of the non-dominant hand. We introduce a microsurgical technique of remote re-vascularisation to reduce cold ischemia time (CIT) of the abdominal wall allograft.. Methods The technique involves primary remote vascularisation of the abdominal wall graft via the vessels of the non dominant forearm (ulnar or radial artery with corresponding venae comitantes). This process is synchronous with the visceral transplant. The graft is transferred onto the recipient’s inferior epigastric (IE) artery after the visceral transplant is done. Conclusions Remote synchronous re-vascularisation of the composite abdominal wall allograft reduces the CIT for the abdominal wall graft. In addition it allows flexibility in the timing of insetting the graft onto the IE or IMA of the recipient. . Fig.1: Composite Abdominal Wall graft Fig.2: Revascularization of the graft using the forearm vessels Fig.3: Preparation of the Inferior Epigastric vessels Fig.4: Final result