Download
1 / 15
170 likes | 1.08k Views
History. First reported in 1908 by Dr.Shanahan, 11 patients who had epileptic seizures.World War I and Vietnam WarA relatively rare form of pulmonary edema, develops within a few hours of well-defined neurologic insult. Clinical presentations. NPE characteristically presents within minutes to hour

E N D
1. Neurogenic Pulmonary Edema
???:Ri ???
2. History First reported in 1908 by Dr.Shanahan, 11 patients who had epileptic seizures.
World War I and Vietnam War
A relatively rare form of pulmonary edema, develops within a few hours of well-defined neurologic insult
3. Clinical presentations NPE characteristically presents within minutes to hours of a severe CNS insult
Sudden onset of dyspnea is the most common symptom; mild hemoptysis may occur as well
Crackles, respiratory distress, normal jugular venous pressure and absence of cardiac gallop
4. Causes Major causes:
Epileptic seizure
Cerebral hemorrhage
Head injury
5. Causes Minor causes:
Multiple sclerosis with medullary involvement
Non-hemorrhagic strokes
Bulbar poliomyelitis
Air embolism
Brain tumors,
Electroconvulsive therapy
6. Frequency In USA, 1/3 of patients with status epilepticus have evidence of NPE
71% of fatal cases of SAH are complicated by NPE
Incidence of NPE is significantly lower in children than in aldults
7. Pathophysiology The exact cause of NPE is unknown
Key etiologic factor:IICP
Animal studies suggest the hypothalamus, medulla(A1,A5), nuclei of solitary tract, area postrema, IICP, activation of sympathetic system have potential roles
8. Mechanism Changes in capillary hydrostatic pressure
LA pressure? because of sympathetic tone?and venous return
LV performance may deteriorate secondary to the direct effect of catecholamines
Pulmonary vasoconstriction ? capillary hydrostatic pressure?
9. Mechanism Changes in pulmonary capillary permeability
Some direct nervous system control over the pulmonary capillary permeability
Epinephrine, norepinephrine, secondary mediators may directly increase pulmonary vascular permeability
10. Workup Lab studies:not helpful
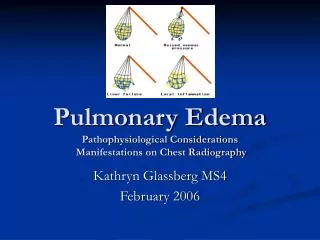
Imaging studies:CXR
Procedures:
Swan-Ganz catheter:systemic blood pressure, cardiac output and pumonary capillary wedge pressure are normal in the time NPE is diagnosed clinically.
11. Differentials Pneumonia, Aspiration
Pneumonia, Bacterial
Pulmonary Edema, Cardiogenic
12. Treatment Supportive and conservative treatment
Focus treatment on the underlying disease
NPE usually resolves within 48~72 hrs
Oxygen is required in most patients
13. Treatment Mechanical ventilation may be necessary, either face mask or ET
GCS score = 8 should be intubated
PEEP with hypocarbia may be required to ?ICP
Tidal volumes set 5~8 ml/kg to avoid excessively high inflation pressure
14. Treatment The peak inspiratory pressure should be kept below 30 cmH2O
ICP monitor is probably appropriate if PEEP exceeds 10 cmH2O
Sufficient cardiac output (cardiac index > 2.2 L/min/m2) and hemoglobin (>10 g/L) are required
15. Treatment Pharmacological agent are not used routinely in treatment of NPE
Alpha blocker can prevent NPE in experimental models, but no human have established the safety and efficacy of these agent
16. Prognosis NPE usually is well tolerated by patient, and usually resolves within 48~72 hrs
Prognosis is determined by the couse of underlying neurological problems
Anesthesiology clinics of North America vol 19. number 2, June 2001
America Rev Respiratory Disease 1978 Oct ; 118(4): 738-6
e-Medicine Specialties, pulmonary edema, neurogenic