Download
1 / 66
660 likes | 831 Views
Quality. Health care seen as a Rubic cube. Quality. The Russian Doll of Health Care. Quality. Just something for health care in developed economies???.

E N D
Quality Health care seen as a Rubic cube
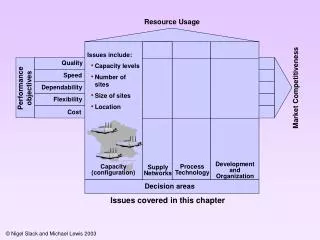
Quality The Russian Doll of Health Care
Quality Just something for health care in developed economies???
“Concern about the quality of care is as old as medicine. But honest concern about quality, however genuine, is not the same as methodical assessment based on reliable evidence”. (Robert Maxwell BMJ 1984)
All health systems have problems • 12% patients suffer from errors caused by health system • International comparisons show deficits in all health systems • Variations within systems • Attention grabbed by head line catastrophic failures of care • Institute of Medicine “Crossing the Chasm”
Challenge …….should you decide to accept it…... • Is to reverse “Institutional Blindness” to problems of quality and safety.
Five themes from 30 enquiries into care disasters in the UK. • Poor communication • Disempowerment of staff and patients • Ineffective systems and processes • Isolation • Inadequate leadership/management
Quality: • Agenda • Management • Benchmarking • Total Quality Management • Industry • Audit
Quality: • Assessment • Assurance • Control • Improvement • Quality vs. Safety • Clinical governance
What else is “quality” • Performance indicators (54) • Standards • Report cards • Public access to performance data • League tables • Comparative health status data
Quality improvement in UK • Confidential enquiry into maternal deaths • Laboratory quality assurance • External inspection residential care homes • CEPOD
Quality improvement in UK • Pre 1989 “Doctor knows best” • 1989 Medical audit • 1991 Clinical audit • 1999 Clinical governance
Quality improvement in the UK • 1996 Calman Hine Cancer report • 1997 Clinical Governance • 1998 NICE and CHI • 1998 National Service Frameworks • 1999 Cancer Care Collaboratives • 2000 An Organisation with a Memory • 2000 NHS 10 year plan much CQI
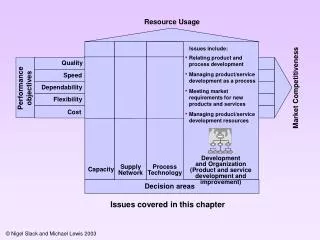
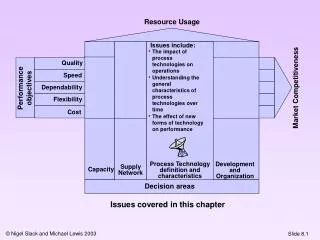
The Rubric Cube – dimensions of quality : (Maxwell BMJ 1984) • Effectiveness • Efficiency • Equity • Appropriateness • Acceptability • Access
More dimensions - for 2006 • Choice • Respect • Provision of “real information” • Safety
Frameworks for assessing quality of care-(Donabedian) • Structure • Process • Outcome • Medical technical • Interpersonal
Everyone talks about it: but no one does anything about it Mark Twain on English weather
Who cares about “quality”? Politicians Purchasers of health care Provider institutions Professionals Public - media Patients
Checking where we are? • Health care system • Interface between organisations • Provider organisation • Interface between clinical services • Clinical teams • Patient - practitioner interface • Or…responding to headlines???
Quality in terms of the system or service: • National/regional waiting lists • Health outcomes • Or …?health outcomes of health care • Provision of specialist services
In terms of hospital or practice: • Access/equity • Process of care for groups of patients • % appropriate use of effective treatments • Efficiency - or costs- or value for money?
In terms of Patient - practitioner interface: • Choice • Access: no waits • Effective treatment/relief • Involvement in decision making • Medico-technical skills of clinicians • Communication skills of clinicians
Quality: • Link between organisational behaviour and clinical practice and health care outcomes • Any improvement in clinical care requires an organisational change.
Quality • Improving the quality of care within current resources. • Making changes that can be shown to improve care for patients • Practical approach to closing gaps between the ideal, what is wanted, what is expected and what is actually happening • Making sure more winners than losers and more winning than losing • Being smart, thinking out of the box and taking others with you
Quality: Balancing needs of populations and individuals • Giving patients a better deal • Always giving THE patient very good care • Some professionals sometimes find this tough
Quality: is about change management • Defining the gaps in care • Understanding the causal problems • Working out a solution • Managing the change • Reassessing the affects of that change
Health leader and quality of care. • Needs to be able to describe the quality of care • Needs mechanisms for further improvement • Needs early warning response mechanisms. • Articulates expectations to employees • Exerts proper role as “employer” • Carries a sense of “ Chronic Anxiety” about the quality and safety of care that is being delivered
Health leader’s role in quality? • Philosopher: having the ideas • Politician: getting the ideas across • Plumber: putting the ideas into action
Philosopher • Set out values • Understand the complexities of the issues • Works out priorities • Relate concerns to practice • Connect between worlds • Reflective part of role
Six worlds:(after Dawson 1997) • Pure science • Clinical trials • Meta analysis • Guidelines and protocols • Organisation • Clinical practitioner
Politician • Translating the philosophy into strategy • Linking external drivers to internal mechanisms • Picking up and responding to concerns • Communicating to many groups • Ensure relevance to everyone involved in change • Understanding the impact on different groups • Ensure local ownership of problem and solutions • Working under constant pressure
Plumber • Managing change • Working through ambiguities • Understanding incentives • Measure results • Working under constant pressure
Plumber’s role: unblocking the system • If you go on doing what you are doing – you go on getting what you’ve got. • Everyone wants to improve – but there are many blocks • Someone is going to have to change how they work
Block 1- demonstrating problem • Evidence of problem or need for change • Acceptance of problem • Ownership of problem • Availability of data • Timeliness of change
Nature of evidence • Often contended/challenged • Plural of anecdotes = data • Has not been reliable or complete or relevant • Need to understand clinical data in the context of organisational practice
Nature of “evidence” of problem • Beyond reasonable doubt:clinical trials • On the balance of probabilities: quality improvement
Block 2 - understanding systems • Complexity of care • Improving the quality of care always involves changing the system of care • Clinical education focussed almost solely on the care of individuals • Little emphasis in education on care of systems
Three central laws of improvement • Results are the properties of systems • Every system is perfectly designed to get exactly the results that it gets. • For every complex problem there is a simple solution: and it is wrong
Blocks 3 - global • Time • Territory • Tradition • Trust • Training
“New clinical skills” - ability to: • Perceive and work in interdependencies • Work in teams • Understand work as a process • Collect and analyse outcome data • Collaborative exchange with patients • Collaborative exchange with lay managers
Quality • Puts values into practice? • Describes clinical practice in organisational terms? • Balances best deals for populations with excellence for individuals?
Quality Workforce + education+ training = Improved quality of clinical care
Assumptions are things that you don’t know you are making. Douglas Adams
Quality improvement in UK • Confidential enquiry into maternal deaths • Laboratory quality assurance • External inspection residential care homes • CEPOD