Download
1 / 39
390 likes | 493 Views
Diabetic Revascularisation. 2002. 3000. 2500. 2000. Type 1. Diabetes prevalence (thousands). Type 2. 1500. 1000. 500. 0. 2010. 2000. 1995. Three million by 2010. Amos AF et al. Diabet Med 1997; 14 (Suppl 5);S1–S85. Obesity and the risk of Diabetes in women. risk.

E N D
3000 2500 2000 Type 1 Diabetes prevalence (thousands) Type 2 1500 1000 500 0 2010 2000 1995 Three million by 2010 Amos AF et al. Diabet Med 1997;14(Suppl 5);S1–S85
Obesity and the risk of Diabetes in women risk Body Mass index
Epidemiology: type 2 diabetes • By 2010, an estimated 3 million people in the UK will have type 2 diabetes1 • Currently 50% of people with type 2 diabetes in the UK are undiagnosed2 • Affects one in 10 older people2 • Occurs more frequently among those of Asian and African-Caribbean descent2 1. Amos AF et al. Diabet Med 1997;14(Suppl 5):S1–S85 2. BDA. King’s Fund. Counting the Cost. 1996
Potential novel risk factors for cardiovascular disease in patients with type 2 diabetes • Inflammation • Fibrinogen • CRP • PAI-1 • Dyslipidaemia • S.-dense LDL • Triglycerides • Low HDL DM type 2 Insulin resistance Hyperinsulinaemia Hyperglycaemia • Fibrinolysis / coagulation • Fibrinogen • PAI-1 • T-pa • Endothelial dysfunction • S.-adhesion-mol • PAI-1 • Oxidative stress • F2 isoprostandes • EO6 epitopes • Ox-LDL • Glycation • AGE proteins • AGE auto-AB
High risk of cardiovascular events in type 2 diabetes - Non-diabetic subjects - Subjects with type 2 diabetes + (based on Haffner et al)
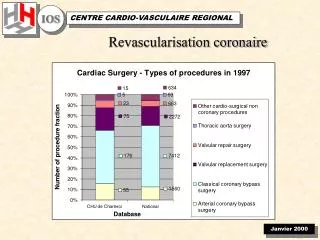
DM:Stent ARTS Trial: 1-Year MACE MACE = Death / MI / CVA / Revascularization Abizaid. Circulation. 2001;104(5):533.
Why are diabetics different ? • Complications • Cardiac • Thromobosis • Restenosis • Extra cardiac • CVA • PVD • Renal
Plaque Compositionand Macrophages in Diabetes Diabetes No Diabetes Moreno. Circulation. 2000;102:2180.
The EPI Trials: 1-Year Mortality by Diabetic Status 4.5% Death (%) 2.6% 2.5% 1.9% P=0.031 Bhatt. JACC. 2000;35(4):922.
The role of GPIIbIIIa inhibitors p = 0.018 88 % reduction Abciximab 0.9 n = 108 1-year Mortality in Diabetics Who Underwent Multivessel Intervention Death 1-year 10 7.7 8 % of Patients 6 Placebo 4 2 0 n = 65 Bhatt et al. JACC 2000;35:922-8
Pooled Data: 1-Year MortalityInsulin-Treated Diabetes 8.1% 4.2% P=0.07 Bhatt. JACC. 2000;35(4):922.
EPIC: 1-Year Mortality metabolic syndrome 5.1% % Patients 2.3% P=0.044 Bhatt. JACC. 2000;35(4):922.
PCI PTCA and Diabetes RestenosisRate (%) 47 71 69 61 61 41 35 53 69 66 63 56 62 Author Holmes et al Vandormael et al Lambert et al Quigley et al Ellis et al Macdonald et al Bourassa et al Weintraub et al Rabbani et al Le Feuvre et al Van Belle et al Levine et al Van Belle et al Year 1984 1987 1988 1989 1989 1990 1991 1993 1994 1994 1997 1997 1998 Van Belle. JACC. 1999;34:476.
Diabetes “Maladaptive” Arterial Remodeling No diabetes Diabetes Kornowski. Am J Cardiol. 1998;81:1298.
IVUS MaladaptiveArterial Remodeling Lesion Reference
SIRIUS Primary Endpoint: 9m Target Vessel Failure. P = <0.001 59% TVF: Target vessel revascularisation, recurrent infarction (Q wave or protocol-defined non-Q wave), or cardiac death that could not be clearly attributed to a vessel other than the target vessel.
SIRIUS: Multivariable Predictors • For all major angiographic and clinical endpoints: • Reference vessel diameter • Lesion length • Diabetes • For both control & CYPHER.
Major Trials Trials to date • BARI 353 • CABRI 122 • EAST 59 • RITA 62 • ERACI (I & II) 90 • ARTS 208 • SOS 150
Major Trials: Revascularisation in allcomers BARI EAST CABRI Trials conducted in either pre- or post- stent era - all comers ARTS Post-coated stent Post-reopro Post-Rx metabolic syndrome ERACI II Pre-stent SOS CARDia Post-stent 1995 2002
CARDia Trial Diabetic patients with multivessel disease or complex single vessel disease No Suitable for PCI or CABG registry No Inclusion and exclusion criteria met registry No registry CONSENT Randomisation CABG PCI +stent Randomisation Bare stent Coated stent
Glasgow Western Hairmyers James Cook University Blackpool Dublin Liverpool Sheffield Nottingham Birmingham Papworth Bristol LONDON Southampton Brighton CARDiaCentres The 6 centres London are: Hammersmith hospital St Mary’s Hospital St Thomas’ Hospital Kings College Hospital London Chest Hospital Harefield Hospital
Joint Prime Sponsor Joint Prime Sponsor Diabetes and Coronary Heart Disease Symposium Wolfson Conference Centre Hammersmith Hospital, London Friday, 1 November 2002 The Diabetic Heart Professor Lars Rydén, Stockholm Benefits of Adjunctive Therapy in DM Vascularisation Professor Nicolas Danchin Nantes Insulin Resistance and CV Risk Dr Miles Fisher, Glasgow Operating on Diabetes Mr Bruce Keogh, Birmingham Dyslipidaemia in Type 2 DM Professor John Betteridge, London Intervention in DM Dr Martyn Thomas, London Diabetic CHD in Asians Dr Adam Timmis, London Hypertension in Type 2 DM Professor Bryan Williams, Leicester CARDia –drug eluting stents in diabetics, Dr Akhil Kapur, London UKPDS and Prevention Professor Rury Holman, Oxford
SIRIUS: Multivariable Predictors of In- Segment Restenosis (CYPHER)
Atherothrombotic components of the Insulin Resistance syndrome Hyper insulinaemia Glucose intolerance Increased Triglyceride INSULIN RESISTANCE PAI-1 T-PA Hypertension Factor VII Factor XII Fibrinogen Key: PAI-1 = plasminogen activator inhibitor-1 t-PA = tissue-type plasminogen activator
Abciximab results • Abciximab with coronary stenting as compared with coronary stenting alone resulted in a significant reduction in the primary end point at 30 days (6.0% vs 14.6%, p=0.01) • The benefit of active treatment at 6monthswith the similar composite of death, reinfarction or urgent revascularisation of target vessel occurring in 7.4% of Abciximab group, as compared with 15.9% in the placebo group (p=0.02) • The clinical outcomes in the abciximab group related to higher frequency of TIMI grade 3 coronary blood flow as compared to the placebo group(before procedure, 16.8%vs. 5.4%; immediately after intervention, 95.1% vs. 86.7%; six months after, 94.3% vs 82.8%, all p< 0.05)
Major Trials Pre-stent versus stent eras • Mortality 1 yr all patients CABG PCI • BARI 3.1% 6.3% • EAST 2.1% 4.5% • CABRI 2.7% 3.9% • ARTS 2.8% 2.5% • ERACI II 7.8% 2.2% • SOS (2yrs) 1.2% 4.1%
Diabetes AMI Angioplasty Diabetes: Urgent PCI Cohort % Patients Age Creatinine EF Multivessel disease Insulin tx DM In-Hospital Mortality Number of Risk Factors n= 45 145 219 147 59 13
4 Diabetes (n=1462) 3.3% 3 No Diabetes (n=5072) 2.1% 2 Death (%) 1 P=0.012 0 0 50 100 150 200 250 300 350 Days From Randomization The EPI Trials: 1-Year MortalityDiabetes vs No Diabetes Bhatt. JACC. 2000;35(4):922.
Peripheral Blood Monocytes NFBp65 Staining Activated NFB: Control Diabetes Bierhaus. Diabetes. 2001;50:2792.