Download
1 / 19
280 likes | 2.22k Views
T.E.N.S. Trancutaneous Electrical Nerve Stimulation. General Concepts:. An Approach to pain control Trancutaneous Electrical Nerve Stimulation: Any stimulation in which a current is applied across the skin to stimulate nerves 1965 Gate Control Theory created a great popularity of TENS

E N D
General Concepts: • An Approach to pain control • Trancutaneous Electrical Nerve Stimulation: • Any stimulation in which a current is applied across the skin to stimulate nerves • 1965 Gate Control Theory created a great popularity of TENS • TENS has 50-80% efficacy rate • TENS stimulates afferent sensory fibers to elicit production of neurohumneral substances such as endorphins, enkephalins and serotonin (i.e. gate theory)
Indications Control Chronic Pain Management post-surgical pain Reduction of post-traumatic & acute pain Precautions Can mask underlying pain Burns or skin irritation prolonged use may result in muscle spasm/soreness caffeine intake may reduce effectiveness Narcotics decrease effectiveness TENS
TENS may be: • high voltage • interferential • acuscope • low voltage AC stimulator • classical portable TENS unit
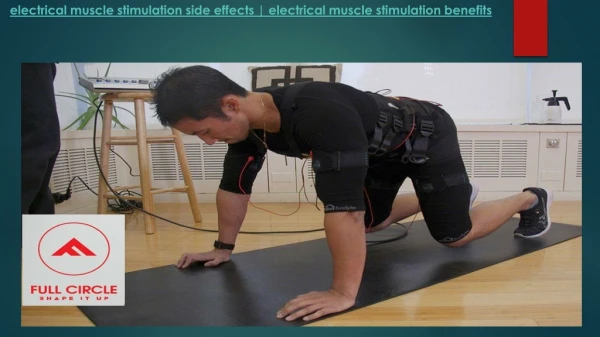
Biophysical Effects • Primary use is to control pain through Gate Control Theory • May produce muscle contractions • Various methods • High TENS (Activate A-delta fibers) • Low TENS (release of -endorphins from pituitary) • Brief-Intense TENS (noxious stimulation to active C fibers)
Techniques of TENS application: • Conventional or High Frequency • Acupuncture or Low Frequency • Brief Intense • Burst Mode • Modulated
Conventional Tens/High Frequency TENS • Paresthesia is created without motor response • A Beta filers are stimulated to SG enkephlin interneuron (pure gate theory) • Creates the fastest relief of all techniques • Applied 30 minutes to 24 hours • relief is short lives (45 sec 1/2 life) • May stop the pain-spasms cycle
Application of High TENS • Pulse rate: high 75-100 Hz (generally 80), constant • Pulse width: narrow, less than 300 mSec generally 60 microSec • Intensity: comfortable to tolerance
Set up: • 2 to 4 electrodes, often will be placed on post-op. Readjust parameters after response has been established. Turn on the intensity to a strong stimulation. Increase the pulse width and ask if the stimulation is getting wider (if deeper=good, if stronger...use shorter width)
Low Frequency/Acupuncture-like TENS: • Level III pain relief, A delta fibers get Beta endorphins • Longer lasting pain relief but slower to start • Application • pulse rate low 1-5ppx (below 10) • Pulse width: 200-300 microSec • Intensity: strong you want rhythmical contractions within the patient’s tolerance
Burst Mode TENS • Carrier frequency is at a certain rate with a built in duty cycle • Similar to low frequency TENS • Carrier frequency of 70-100 Hz packaged in bursts of about 7 bursts per second • Pulses within burst can vary • Burst frequency is 1-5 bursts per second • Strong contraction at lower frequencies • Combines efficacy of low rate TENS with the comfort of conventional TENS
Burst Mode TENS - Application • Pulse width: high 100-200 microSec • Pulse rate: 70-100 pps modulated to 1-5 burst/sec • Intensity: strong but comfortable • treatment length: 20-60 minutes
Brief, Intense TENS: hyper-stimulation analgesia • Stimulates C fibers for level II pain control (PAG etc.) • Similar to high frequency TENS • Highest rate (100 Hz), 200 mSec pulse width intensity to a very strong but tolerable level • Treatment time is only 15 minutes, if no relief then treat again after 2-3 minutes • Mono or biphasic current give a “bee sting” sensation • Utilize motor, trigger or acupuncture points.
Brief Intense TENS - Application • Pulse width: as high as possible • Pulse rate: depends on the type of stimulator • Intensity: as high as tolerated • Duration: 15 minutes with conventional TENS unit. Locus stimulator is advocated for this treatment type, treatment time is 30 seconds per point.
Locus point stimulator • Locus (point) stimulators treatment occurs once per day generally 8 points per session • Auricular points are often utilized • Treat distal to proximal • Allow three treatment trails before efficacy is determined • Use first then try other modalities
Modulated Stimulation: • Keeps tissues reactive so no accommodation occurs • Simultaneous modulation of amplitude and pulse width • As amplitude is decreased, pulse width is automatically increased to deliver more consistent energy per pulse • Rate can also be modulated
Electrode Placement: • May be over the painful sites, dermatomes, myotomes, trigger points, acupuncture points or spinal nerve roots. • May be crossed or uncrossed (horizontal or vertical
Contraindications: • Demand pacemakers • over carotid sinuses • Pregnancy • Cerebral vascular disorders (stroke patients) • Over the chest if patient has any cardiac condition