Download
1 / 43
430 likes | 455 Views
This unit focuses on the design features, strengths, and limitations of case-control, case-crossover, and cross-sectional studies in public health research. It covers topics such as biases, prevalent vs. incident cases, control group selection, and more. Case-control studies entail defining cases, selecting controls, comparing exposures, and calculating odds ratios. Issues like disease duration determinants, recalling events, and disease development are explored, emphasizing the importance of selecting cases and controls carefully. Various sources of cases and controls, ascertainment of disease status, and selection biases are discussed. The unit also delves into prevalent vs. incident cases, highlighting the challenges and circumstances where prevalent cases are preferred. Overall, it aims to equip learners with a comprehensive understanding of conducting case-control studies effectively.

E N D
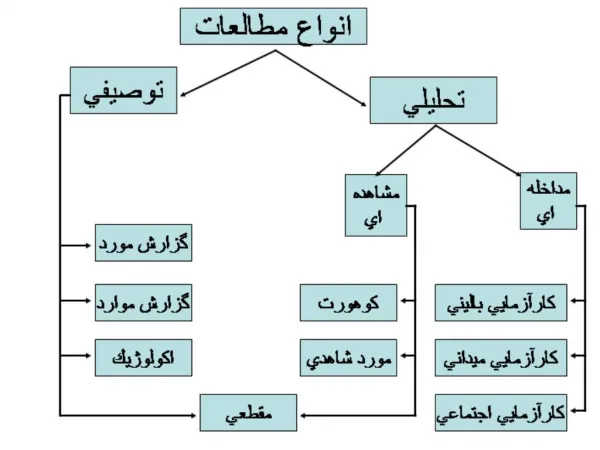
Unit 10: Case-Control, Case-Crossover, and Cross-Sectional Studies
Unit 10 Learning Objectives: • Understand design features of case-control, case-crossover, and cross-sectional studies. • Understand strengths and limitations of case-control, case-crossover, and cross-sectional studies. • Recognize potential biases from case-control, case-crossover, and cross-sectional studies. • Recognize the impact of using prevalent versus incident cases in case-control studies. • Recognize the difficulty in selecting an appropriate control group in case-control studies. • Understand the nested case-control study design. • Recognize the difference between fixed and time-dependent variables, including confounding variables.
Case-Control Studies
Case Control Studies PRIMARY STEPS: • Define and select the cases. • Assemble an appropriate comparison group (controls). • Determine and compare the proportion of cases who have experienced the exposure of interest -- with the proportion of controls who experienced the exposure.
Case Control Studies • Typically, compare the proportions of exposure by means of a ratio: ODDS RATIO OR = Odds for exposure among cases Odds for exposure among controls (a / c) OR = ------- (b / d)
Defining Cases • Ensure cases are as homogenous as possible. Establish strict diagnostic criteria (e.g. certain histologic characteristics). • Sub-definitions of cases such as definite, probable or possible may be needed. • Analysis can be conducted for each sub-group.
Prevalent vs. Incident (Newly Diagnosed) Cases To the extent possible, avoid including prevalent cases! WHY?
Prevalent vs. Incident (Newly Diagnosed) Cases Why? • Determinants of disease duration may be related to the exposure such that the magnitude of the exposure (e.g. low vs. high) may be inaccurate. • Prevalent cases with long disease duration may not accurately recall antecedent events.
Prevalent vs. Incident (Newly Diagnosed) Cases Why? • With prevalent cases, it is more difficult to ensure that reported events preceded disease development rather than being a consequence of the disease process.
Prevalent vs. Incident (Newly Diagnosed) Cases ---However, case-control studies of congenital malformations are inevitably based on prevalent cases. ---Prevalent cases are commonly used in studies of chronic conditions with ill-defined onset times (e.g. multiple sclerosis).
Selecting Cases • Sources of Cases: • Hospitals, medical care facilities, etc. • General population - locate and obtain data from all or a random sample of individuals from a defined population.
Selecting Cases • Note: DO NOT compromise validity in the goal of generalization. • Select cases from a defined population in whom complete and reliable information can be obtained, and where the exposure/disease relationship is presumed to be present.
Defining and Selecting Cases • Ascertainment of Disease Status: • Case registries (i.e. cancer) • Office records of physicians • Hospital admission or discharge records • Pathology department log books
Selecting Controls • Axiom: Selection of an appropriate comparison group is the most difficult and critical issue in the design of case-control studies.
Selecting Controls • Controls are subjects free of the disease (or outcome of interest). • Controls are seldom subjected to medical exam to rule out the disease of interest. • Usually, they are assumed disease free if they have not been diagnosed.
Selecting Controls 1. The prevalence of exposure among controls should reflect the prevalence of exposure in the source population. 2. Controls should come from the same source population as cases (e.g. would have been cases if diagnosed with the disease).
Selecting Controls 3. The time during which a subject is eligible to be a control should be the time in which the individual is also eligible to be a case. If #1, #2, or #3 are not met = Selection Bias
Selecting Controls Sources of Controls: --- General population --- Random digit dialing --- Neighborhood --- Friends/relatives --- Hospital or clinic-based
Selecting Controls General Population Controls: --- Population defined by geographic boundaries (or specific characteristics). --- Cases may include all cases, or a random sample of all cases. --- Controls should be a random sample of non-diseased individuals eligible to be cases.
Selecting Controls General Population Controls: --- If entire population is sampled for cases and controls, can calculate incidence rates of disease in exposed and non-exposed. --- Selection of controls may be costly, time consuming, and exposure recall may not be as accurate as “sick” controls. --- Subjects in general population may be less motivated to participate than hospital-based controls.
Selecting Controls Random Digit Dialing Controls: --- May approximate random sampling from the source population. --- Controls are often matched to cases on area code and prefix (i.e. SES matching). --- Probability of contacting each eligible subject may differ due to time of day, number in household, answering machines, etc.
Selecting Controls Neighborhood Controls: --- May approximate random sampling from the source population. --- Controls are often matched to cases from the same neighborhood. --- If cases are from a particular hospital, neighborhood controls may include people who would not have been treated at the same hospital had they developed the disease (e.g. VA hospital).
Selecting Controls Friend/Relative Controls: --- Tend to be more cooperative than general population controls. --- Often similar to cases on factors such as SES, lifestyle, and ethnic background. --- However, being named as a friend by the case may be related to exposure status of the potential control.
Selecting Controls Friend/Relative Controls: --- The list of potential friend/relative controls is often derived from the case; this dependence may add a potential source of bias. --- Hence, friend/relative controls may be too similar to cases regarding the exposure of interest.
Selecting Controls Hospital/Clinic-Based Controls: --- Source population refers to people who “feed” the hospital or clinic. --- Usually easier and less expensive than general population controls. --- May be more aware of exposures and likely to cooperate than general population controls (healthier).
Selecting Controls Hospital/Clinic-based Controls: --- Controls are ill; distribution of the exposure may not reflect the distribution of exposure in the source population for cases. --- Controls should be limited to diagnoses for which there is no prior indication of a relation with exposure. --- Subjects may have changed their exposure status as a result of being sick.
Selecting Controls General Remarks: --- Often, there is no perfect control group; several groups can be selected, if feasible. --- If study results are consistent across control groups, may indicate a valid result, but also possibly similar net bias. --- If different effects are observed, may provide useful information as to nature of the association or potential biases.
Selecting Controls For each control group, how many controls per case? -- the optimal case-control ratio is 1:1 -- when the number of cases is small, the sample size for the study can be increased by using more than one control e.g. 1:2 1:3 1:4
Selecting Controls AXIOM: The benefit of increased sample size is not as relevant past the 1:4 ratio (e.g increase in statistical power).
Ascertaining Exposure • Sources of exposure data (cases and controls): ---Study subjects (self-report). Particularly vulnerable to recall bias as cases may recall their exposure history more thoroughly than controls. ---Records (preferably completed before the occurrence of outcome events). ---Interviews with surrogates (spouses, siblings, etc.).
Ascertaining Exposure • How far back should exposure be assessed? ---Define a part of the person’s exposure history considered relevant to the etiology of disease (e.g. the “empirical induction” period). ---Code the exposure data in an etiologically-relevant manner (e.g. magnitude of exposure, years of exposure, ever exposed, etc.).
Nested Case-Control Study Definition: Hybrid design in which a case- control study is nested in a cohort study. Exposure Status Ascertained Cohort Study Population Subjects Develop Disease Do Not Develop Disease CASES CONTROLS
Nested Case-Control Study Advantages: ---Exposure data are collected before disease development; eliminates recall bias. ---Can be economical if complete exposure ascertainment is limited to only cases and controls nested in the total cohort. Often used in occupational epidemiology where the occupational cohort is the source population.
Summary – Case Control Studies ---Selection of an appropriate comparison group is the most challenging and important aspect of the study design. ---In population-based studies, incidence can be calculated when entire population is sampled. ---Hospital-based studies are often easiest and cheapest to conduct, but may be prone to biased exposure ascertainment.
Summary – Case Control Studies Advantages: ---Relatively quick and inexpensive. ---Well suited to evaluation of diseases with long induction periods. ---Optimal for evaluation of rare diseases. ---Can examine multiple etiologic factors for a single disease.
Summary – Case Control Studies Disadvantages: ---Inefficient for evaluation of rare exposures unless the disease is common among the exposed. ---If not population based, cannot compute incidence among the exposed and non- exposed.
Summary – Case Control Studies Disadvantages (cont.): ---May be difficult to establish the temporal relationship between exposure and disease. ---Prone to bias compared to other analytic designs, in particular, selection and recall bias.
Review of Recommended ReadingPPA and Risk of Hemorrhagic Stroke --- Case control study investigating exposure to products containing phenylpropanolamine (PPA) and risk of hemorrhagic stroke in persons 18-49 years of age. --- 702 cases and 1,376 matched control subjects (random-digit dialing) from 43 hospitals in 4 states (1994 to 1999) --- Multiple definitions of exposure to PPA, including any use, first use, specific type of product (i.e. appetite suppressant). --- Primary focal time to assess prior exposure history was day/time that symptoms led subject to seek medical attention. --- Trained interviewers used structured instrument to document prior exposure history. --- Analyses conducted separately for men and women.
Discussion Question 1 The investigators excluded stroke victims who died or did not have the ability to communicate because they felt that proxy data (i.e. spouse) on exposure status would be unreliable. How might this exclusion of potential case subjects bias (if at all) the study results? Source: NEJM 2000; 343:1826-1832.
Discussion Question 2 The primary time in which exposure to PPA was assessed occurred immediately preceding the time in which medical attention was sought. What type of bias (if any) could this strategy have introduced? Source: NEJM 2000; 343:1826-1832.
Discussion Question 3 On average, cases were required to recall PPA exposure status over a more remote period than control subjects. Do you think this strategy offset the potential greater motivation for cases to recall exposures to over-the-counter medications than control subjects? Source: NEJM 2000; 343:1826-1832.
Discussion Question 4 Not stated in the article, the participation rate for eligible subjects was 75% for cases compared to 36% for controls. How might this differential rate of participation bias (if at all) the study results? Source: NEJM 2000; 343:1826-1832.
Discussion Question 5 Interpret the results in table 4. Are the findings similar among men and women? Source: NEJM 2000; 343:1826-1832.