Download
1 / 26
260 likes | 536 Views
Anatomy and histology of genital tract & physiology of menstruation. Dr. Sura Findakly MBChB , DGO, CABOG. Learning objectives:. Describe the anatomical structure and histology of the organs of the female reproductive system

E N D
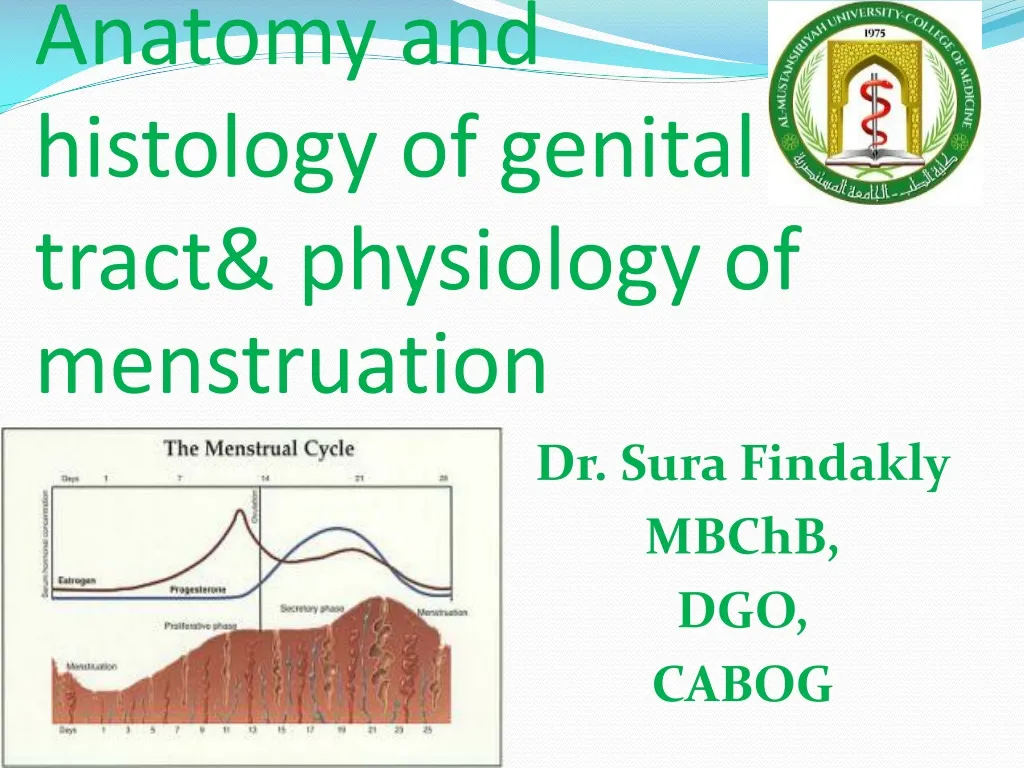
Anatomy and histology of genital tract& physiology of menstruation Dr. SuraFindakly MBChB, DGO, CABOG
Learning objectives: • Describe the anatomical structure and histology of the organs of the female reproductive system • Recognize the hormonal changes that occur during the ovarian and endometrial cycles.
Anatomical overview of the ovary The human ovary volume average 3,2, and 1 cm. it is freely mobile white to gray in color, lying on the posterior abdominal wall suspended by the strong suspensory ligament of the ovary. The ligament passes very closely to the bifurcation of the common iliac artery and uretermaking it liable to injury during hysterectomy. Blood supply of ovary direct branches from the aorta and inferior vena cava.
Ovary histology: 1. Primordial ovarian follicle an ova surrounded by single columnar epithelium. 2. Secondary ovarian follicle which is an ova surrounded by 2 layers of epithelial tissue 3. Tertiary ovarian follicle starts to develop cavity in which colorless fluid 4. Immature Graph Follicles are macroscopic usually 1-3 per each ovary. The fluid filed cavity has enlarged further in exponential way reaching any size up to 18 mm
Ovary histology: 5. Mature Graph follicle between 18-22 mm start to secret estrogen only. Estradiol the most potent estrogen. Those cells undergo further differentiation are Granulosa Cells prime the endometrial lining at day 3 up to the day of ovulation(subtracting 14 days from the expected cycle. 6. Corpus luteum(macroscopic) arises by rupturing the mature Graph Follicle. Corpus lueum is seen as solid body yellow in color and has undulated surface.. The cells of normal graph follicle are converted into lutem cell which differs by being capable of secreting both estradiol and progesterone. Luteinization of the follicular cells. The hypothalamus reduce its frequency while the amplitude of the single wave of GnRH is increased rapidly. At day 21 of 28 days cycle woman the peak serum progesterone and negative estrogen is reached. At this level once Human Chorionic Gonadotrophin is not detected the feedback of released progesterone- estrogen down regulates again for a new cycle and their levels drops gradually so exactly after 14 days a new cycle restart. 7.Corpus albicans
Anatomical overview of the uterus a pear shaped hollow structure which has slit like cavity. Size of the uterus is about 7, 5, 3 cm and enclosed in the broad ligaments. The main body of the uterus is subdivided into 2 parts the uterine body and cervix. The junction between them is the internal os. Internal os remain closed throughout pregnancy and normal cycle. The uterine wall has 3 layers 1. the endometrial lining. 2. The uterine smooth muscle has strong interdegetating fibers 3. The outer layer or serosa has many reflections like vesicouterine reflection. • Blood supply comes mainly from the anterior branch of internal iliac artery. Ureter in each side passes directly under uterine artery near uterus. This water under bridge is close to the uterus which makes them liable to injury during cesarean and hysterectomy. While the sacral plexus at level s2, s3 and s4 is the main nerve supply via the 2 obturator nerve ganglions each on either side near the ischial spine.
Endometrial changes during normal cycle • The follicular or proliferative phase occurs when the ovary is developing the primordial ovarian follicles into 1 single mature follicle. In this phase the endometrium is under estrogen only. The amorphous material between the surface epithelium and the basement membrane starts to increase in thickness gradually. From the surface epithelium few ducts start to appear and go deeper with primitive glandular adenoid structures. The amorphous layer contains few fibroblasts which increase gradually in numbers. The spiral vessels are initially few and less coiled yet gradually increase in number as well as in coiling with advent of follicular phase. • Luteal phase or secretory witness huge increase in the number of mature glandular tissue with well defined adenoids which has typical appearance of adenoma like tissue. The number and coiling of the spiral arterioles increase greatly while fibroblast in the amorphous layer increases hugely in number. This tissue style typical of adenoid appearance is the endometrium which has high affinity to implant the growing embryo.
Anatomical overview of the fallopian tubes • Fallopian tubes are the first uterine structures which deal with the mature released ova. The ova which released from the ovary usually surrounded by a cellular layer called zonapellucida. Some follicular cells may remain attached to it. The fambrial projections around the time of ovulation overlie the ovary with dominant follicle and pick up released ovum into infundibullar part and later to ampullary part of the tube. Then enter the narrow isthmus part end the interstitial part before reaching endometrial cavity where either zygote is implanted or ova die. The ciliary movement of the tube as well as the implantation of zygote occur around day 21 of the cycle and require high serum progesterone.
Simple test to confirm ovulation • Body temperature rise above baseline by 0.5 degrees. • Spinbarkeittest as the cervical mucus is first aspirated. Under high serum estrogen it is widely stretchable while under serum progesterone it becomes thick less stretchable and break easily. Usually done at day 21 of the cycle • Vaginal cells aspiration and staining with eosin and hematoxylin. The cells are acidic or red in color in follicular phase and become blue in mid lutealfase • Aspiration of the endometrial lining for histopathology by bed side method. Various outpatient delicate probes and hollow aspirators are used to obtain endometrial cells without need for anesthesia for histopathology to determine its type. • Serum progesterone at day 21 or mid luteal phase above 20 ug/ ml is highly associated with ovulation. • Ultrasounds scan at day 14 and 21 of the cycle. Finding ovarian follicle 18 mm and above is indication of full follicular maturation while endometrial thickness 4- 5 mm is a strong indicator of ovulation associated with secreteory phase. • The modern widely used kits which stains according to the instructions coming with those kits may be used. Those are urinary sample indicators of progesterone metabolites or even antibodies to LH urinary secretions. The color of the strip is designed to assess roughly serum progesterone.
Squamocolmnar junction and uterine cervix • The cervix is 1-3 cm firm tube shaped with body rich in collagen fibers in addition to muscle projecting into the upper vagina. • It is lined with single columnar epithelium and goblet cells. At the external os it a region called squamo columnar junction the epithelium changes to stratified squamous epithelium. This junction is the site from which carcinoma commonly arise. Screening is done by taking scraps of those cells with wood spatula for pap stain. This condition is called cervical intra epithelia neoplasia. Premalignant cells may be treated with excision of the junction or local destructive therapy by heat, cryocautery, laser and loop excision. Human papilloma virus infection plays a major role in this transformation.
Menstruation definition Monthly shedding of endometrial dead tissue. Menstrual blood is a mixture of dead endometrial tissue, blood components and pus cells. Normal 3-7 days in duration, with frequency 21- 35 days with average 28 days. The total blood loss should not exceed 70- 80 ml and usually above 30- 40 ml.
The hypothalamus and pituitary hormones inducing menstruation • GonadotophinRleasing Hormone or GnRH. in pulsatile manner. • In the follicular phase only FSH is stimulated while in the luteal phase both FSH, LH are secreted. • Normally estrogen and progesterone have strong negative effect on FSH, LH secreting cells. However transition from the follicular phase to the luteal phase passes through short period in which the effect become strongly positive. This heralds the LH/FSH surge in which a sudden increase in the frequency and amplitude of the hypothalamus- pituitary gland. During this short phase rupture of the mature follicle occur and ovulation is induced. • Dopamin has strong inhibitory effect of the prolactin secreting cells . Drug like mtoclopromide, stress and eating disorders greatly inhibits dopamin synthesis and secretion. This may cause amenorrhea.
Phases of human menstrual cycle 1. The follicular phase: • A single primordial follicle fully matured 18- 22 mm diameter. The changes are all brought about by FSH from the pituitary. The uterus lining is re grown by the estrogen which is secreted from the follicle itself. Normally the correlation between estrogen and FSH is negative feedback mechanism. However for very short period this correlation becomes positive leading to ovulation with start of the second phase of the ovary.
Phases of human menstrual cycle Ovulation: • Brief increase in the frequency and amplitude of the GnRH at the hypothalamus and release of FSH, LH Rupture of mature follicle converting the follicle into corpus luteum, which start to secrete estrogen and progesterone.
Phases of human menstrual cycle 2. The luteal phase: • luteal phase age is only 14 days. • During this period the endometrial lining is converted into the secretory which is the only one compatible with implantation of 8- 16 cell stage embryo. • Should pregnancy fail gradually the amplitude as well as the frequency of GnRHdecline menstruation. • Luteal phase is associated with a increase in the temperature about 0.5 degrees above the base line this rise in the temperature remain until the end of the luteal phase.
Ischial spine which is situated between greater and lesser notches. Those notches are converted into two foramen the greater sciatic and lesser sciatic foramen by the sacrospinal ligament and the sacrotuberous ligaments. The Ischial spine in female pelvis is usually small and everted. Nerve and vessels which has to exit the true pelvic cavity into the perineum has to hook around the ischial spine and enter the perineum through the lesser sciatic notch. Mainly the pudendal vessels and nerve. fusion of three bones (ilium, ischium and pubis). Their fusion leaves a large obturatorformaen. has a defect in the anterior part called the obturator canal through which the obturator artery, vein as well as nerve exit the true pelvic cavity to supply the obturator groups of muscles which have internal rotation as well as internal abduction of the thigh.
The cardinal ligament of the pelvis is a unique ligament which has a fan shaped appearance and extends from the pelvic side wall and inserted directly into the lower part of the uterus exactly at the same level of internal os which herald the beginning of the cervical canal.
The levatorani or pelvic floor muscle is the main muscle of the pelvis in female. They are fan shaped extension from the pelvic side wall to meet in the mid line. In the anterior part a defect is present to allow the passage of urethra, vagina as well as the rectum. This defect is called the urogenital hiatus. Each half of this large muscle is composed of 3 pairs of the followings Puborectalis muscle Pubococcygeous muscle Iliococcygeous muscle In addition to those 3 pairs further 2 pairs of Coccygeous muscle Piriformis muscle Have further action full separation of the pelvic cavity from the perineal cavity. In addition to that the 2 sphincter muscles sphincter ani and sphincter urethrae are blended with the fiber of this muscle. The levatorani is composed of striated voluntary muscle fibers, this muscle is the main base for all the pelvis viscera to rest on it firmly.
The vascular supply and drainage of the pelvis is so extensive and huge to the extent that ligation of the internal iliac artery on bilateral basis has no effect on any organ as far as blood supply is concerned. This is mediated by the vast anasthomosis of pelvic blood supply with other major vessels whether before the pelvis, or at the level of pelvis or even beyond the level of pelvis The main blood supply to the pelvis internal iliac artery which gives branches as follows Uterine artery Vaginal artery Superior and inferior vesical artery Lateral sacral artery Middle rectal artery Obturator artery Pudendal artery
The venous drainage of the pelvis is also unique in the form that bladder wall, uterine wall as well as rectum wall contains extensive venous pampiniform plexus which drains gradually to veins with names similar to the counterpart artery and ultimately drains into the internal iliac artery and common iliac artery and inferior vena cava. Branch of the internal iliac artery are the obturator artery and pudendal artery. The obturator artery exits the pelvic cavity through the obturator canal while the pudendal artery leaves the pelvic cavity to enter perineal cavity through hocking around the ischial spine. Its name changes to the lateral perineal artery and after supplying the perineal body it terminates either in the corpus spongiosm under the clitoris or corpora cavernous each one under the labia major fold.
The bladder is covered with peritoneal surface as it is taken from anterior pelvic wall to reach the anterior surface of the uterus at the vesico uterine reflection. The sphincter urethrae muscle is composed of internal smooth muscle fibers and outer striated muscle fibers and blend with the levatorani. Parasympathetic stimulation will result in opening the internal part of the sphincter and contraction of the detrusor muscle. This reflex is at the level of s2, s3 and s4. The uterine body is contained within a large fold of peritoneum which is called the broad ligament. The round ligament arises from the uterine body and after a long course covered with peritoneal fold enters the inguinal canal to be inserted after exit into the labia majora base. Next the ovarian ligament arises from the uterine wall and attached to the ovary. On the to reflexion of the broad ligament the Fallopian tubes appear from lateral fambrial part, ampullary part ischemic part to the uterine cavity. Posterior two ligaments called uterosacral ligament and arise from the level of internal os and inserted into the sacrum. This arrangement leaves a potential cavity behind the uterine wall called the pouch of Douglas.
The perineal body - a condensation of fiber tissue and muscular tissue from. 1. Sphincter urethrae 2. Sphincter anus 3. Levatorani 4.Deep and 5.Superficiall transverse perineal muscles -is the main organ which keeps the rectum separated from the vagina.
The monsveneris is a fatty tissue condensation over the pubic symphsis The clitoris is a distensible projection lie in the upper part of the vulva. During sexual arousal it becomes enlarged due to the presence of corpus spongiosum bellow it Labia major in each side which harbors the Bartholin gland in each. Their openings are bellow The labia minora are usually small fold of thin red skin below which a fatty tissue. Vestibule is the space between the 2 labia minor Bulbs of the vestibule paired of erectile tissue which lie medial aspect of labia minor and enlarge by the underlying corpora cavernosa spongy tissue Greater vestibular glands are pairs of glands posterior to the bulb of the vestibule which secretes mucous around sexual arousal Fourchete is the meeting point of each labia posterior to the vestibule
Lymphatic drainage of the vulva Lymphatic drainage of the vulva usually ends in the superficial and deep lymphatic nodes of the femur. The deep node is a single lymphatic node lays in the inner most compartment of the femoral sheath followed by the femoral vein in the middle and femoral artery in the outer compartment. The femoral nerve passes outside the femoral sheath. This arrangement of lymphatic drainage should be considered in carcinoma of the vulva where in addition to excision of the whole vulva, those lymph nodes should be removed as well otherwise distant metastasis is inevitable.
SUMMARY: Knowing anatomy , histology of female genital tract and physiology of menstruation to diagnose any disease or abnormality and so prevent any complication from happening .