Download
1 / 1
10 likes | 125 Views
SIMULTANEOUS COEXISTENCE OF GH-SECRETING PITUITARY ADENOMA, MENINGIOMA AND CAROTID ARTERY ANEURYSM

E N D
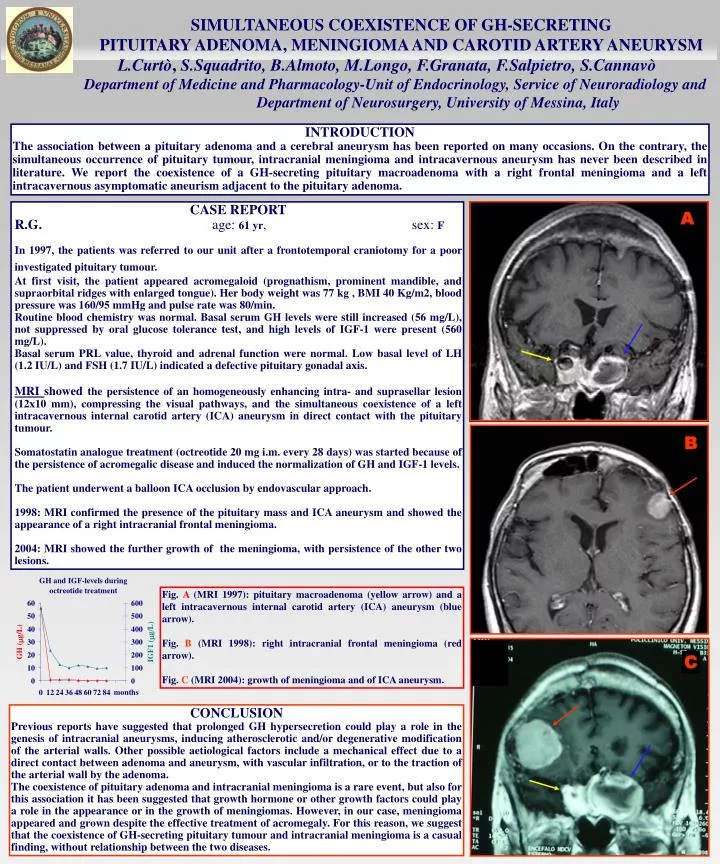
SIMULTANEOUS COEXISTENCE OF GH-SECRETING PITUITARY ADENOMA, MENINGIOMA AND CAROTID ARTERY ANEURYSM L.Curtò, S.Squadrito, B.Almoto, M.Longo, F.Granata, F.Salpietro, S.Cannavò Department of Medicine and Pharmacology-Unit of Endocrinology, Service of Neuroradiology and Department of Neurosurgery, University of Messina, Italy B INTRODUCTION The association between a pituitary adenoma and a cerebral aneurysm has been reported on many occasions. On the contrary, the simultaneous occurrence of pituitary tumour, intracranial meningioma and intracavernous aneurysm has never been described in literature.We report the coexistence of a GH-secreting pituitary macroadenoma with a right frontal meningioma and a left intracavernous asymptomatic aneurism adjacent to the pituitary adenoma. CASE REPORT R.G. age: 61 yr, sex: F In 1997, the patients was referred to our unit after a frontotemporal craniotomy for a poor investigated pituitary tumour. At first visit, the patient appeared acromegaloid (prognathism, prominent mandible, and supraorbital ridges with enlarged tongue). Her body weight was 77 kg , BMI 40 Kg/m2, blood pressure was 160/95 mmHg and pulse rate was 80/min. Routine blood chemistry was normal. Basal serum GH levels were still increased (56 mg/L), not suppressed by oral glucose tolerance test, and high levels of IGF-1 were present (560 mg/L). Basal serum PRL value, thyroid and adrenal function were normal. Low basal level of LH (1.2 IU/L) and FSH (1.7 IU/L) indicated a defective pituitary gonadal axis. MRI showed the persistence of an homogeneously enhancing intra- and suprasellar lesion (12x10 mm), compressing the visual pathways, and the simultaneous coexistence of a left intracavernous internal carotid artery (ICA) aneurysm in direct contact with the pituitary tumour. Somatostatin analogue treatment (octreotide 20 mg i.m. every 28 days) was started because of the persistence of acromegalic disease and induced the normalization of GH and IGF-1 levels. The patient underwent a balloon ICA occlusion by endovascular approach. 1998: MRI confirmed the presence of the pituitary mass and ICA aneurysm and showed the appearance of a right intracranial frontal meningioma. 2004: MRI showed the further growth of the meningioma, with persistence of the other two lesions. Fig. A (MRI 1997):pituitarymacroadenoma(yellow arrow)and a left intracavernous internal carotid artery (ICA) aneurysm (blue arrow). Fig. B (MRI 1998): right intracranial frontal meningioma (red arrow). Fig. C (MRI 2004): growth of meningioma and of ICA aneurysm. C CONCLUSION Previous reports have suggested that prolonged GH hypersecretion could play a role in the genesis of intracranial aneurysms, inducing atherosclerotic and/or degenerative modification of the arterial walls. Other possible aetiological factors include a mechanical effect due to a direct contact between adenoma and aneurysm, with vascular infiltration, or to the traction of the arterial wall by the adenoma. The coexistence of pituitary adenoma and intracranial meningioma is a rare event, but also for this association it has been suggested that growth hormone or other growth factors could play a role in the appearance or in the growth of meningiomas. However, in our case, meningioma appeared and grown despite the effective treatment of acromegaly. For this reason, we suggest that the coexistence of GH-secreting pituitary tumour and intracranial meningioma is a casual finding, without relationship between the two diseases.






