Download
1 / 54
540 likes | 731 Views
A Clinicians Guide to Tick Borne Infections . Alan M. Sanders Upstate Infectious Diseases Associates Albany, N.Y. Introduction to the Tick-borne Diseases. The Vectors and Pathogens. Human Tick-borne Diseases.

E N D
A Clinicians Guide to Tick Borne Infections Alan M. Sanders Upstate Infectious Diseases Associates Albany, N.Y.
Introduction to theTick-borne Diseases The Vectors and Pathogens
Human Tick-borne Diseases Each of the specific infections are associated with a host of potentially related symptoms, yet have unique features that should allow the clinician the opportunity to make: an accurate diagnosis prescribe an appropriate course of antibiotics achieve a timely cure in all patients
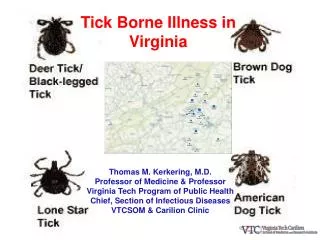
Human Tick-borne DiseasesIn the United States An array of regional tick species in the United States are responsible for the transmission of a wide variety of infections to human hosts: Rickettsial Rocky Mountain Spotted Fever (Rickettsia rickettsii) Human Monocytic Ehrlichiosis (Ehrlichia chaffeensis) Anaplasmosis (Anaplasma phagocytophilum) (also known as Human Granulocytic Anaplasmosis HGA) Spirochetal Lyme Disease (Borrelia burgdorferi) Parasitic Babesiosis (Babesia microti)
Human Tick-borne Diseasesin the United States cont. Tularemia (Tularemia francesis) STARI – Southern Tick Associated Rash Illness Tick-borne Relapsing Fever – (Borrelia species) NOTE: Bartonella infections have not been proven to be tick - associated
Human Tick-borne Diseases:A Focus on the Capital Region of New York State Lyme Disease Anaplasmosis Babesiosis Human Monocytic Ehrlichiosis
Update on Epidemiology Tick-borne Diseases in New York State and the Capital Region
Lyme and other Tick-borne Diseases Incidence New York State 2007-11Excludes NYC. 2011 data provisional. Sources - CDC, NYSDOH.
Tick-borne Diseases Excluding Lyme Disease in New York State2007 (Cases – 452) to 2011 (Cases – 730)Excludes NYC. 2011 data provisional. Sources - CDC, NYSDOH.
Capital Region Lyme Disease Reported CasesAlbany, Columbia, Greene, Rensselaer, Saratoga and Schenectady Counties
Lyme Disease Clinical Features Diagnosis Treatment
Lyme Disease:Objectives • Provide a more sound approach to the diagnostic work-up of Lyme Disease • Review the current serologic tests, and their contribution to accurate diagnoses. • Recognize the limited utility of serologies in a disease that by in large depends upon a clinical diagnosis.
Clinical Stages of Lyme Disease EARLY LOCALIZED Days to Month post tick bite EARLY DISSEMINATED Weeks to Months post tick bite LATE LYME DISEASE Months to Years post tick bite
Early Localized Lyme DiseaseDays – One Month ERYTHEMA MIGRANS (EM) May occur in 80% “Cellulitis” in an atypical locale May see a necrotic center ASSOCIATED SYMPTOMS Fever Flu symptoms Adenopathy Headache
Early Disseminated Lyme DiseaseWeeks - Months CARDITIS 5% untreated patients AV blocks/Cardiomyopathy/Myopericarditis NEUROLOGIC 15% untreated patients Lymphocytic meningitis, encephalitis, cranial neuropathy (III, VI, VII), radiculopathy SKIN Days to weeks after EM with multiple irregular sized lesions
Late Lyme Disease MUSCULOSKELETAL Seen in about 10% of untreated patients Mono-oligoarticular arthritis - mostly knee(s) Expect 20-30K PMN-predominant joint fluid May include chronic synovitis or a Baker’s cyst CUTANEOUS Acrodermatitis chronica atrophicans Morphea-like lesions (Europe) NEUROLOGIC ? incidencebecause few cases Encephalomyelitis (cognitive), peripheral neuropathy
Lyme Disease Diagnostics Clinical diagnosis with serologic confirmation for all stages of Lyme Disease ELISA screening and Western Blot IgM & IgG for confirmation utilizing CDC criteria C6 antibody testing may assist with equivocal WB results Fluid analysis for serologic testing and PCR Detection in synovial and CSF samples
LYME TESTING SUPPORTIVE – NOT DIAGNOSTIC • As with most serologic tests, the pre-test probability of the disease must be considered. • IDSA and ACP guidelines have both concluded that a clinician should NOT test a patient in whom the assessment does not suggest a high likelihood of Lyme (<20%) • A positive serologic test does not constitute proof of active Lyme Disease without clinical support.
SEROLOGIC TEST FOR LYMEA TWO-TIER APPROACH • FIRST TIER TESTING- ELISA or IFA which are very sensitive (re: false +). • IF A FIRST TIER TEST IS NEGATIVE- NO ADDITIONAL TESTING IS NEEDED. • SECOND TIER TESTING – WESTERN BLOT for both IgM and IgG. Indicated for both equivocal and positive ELISA/IFA. • Inter-laboratory variability exists for both tests, notably with WB interpretation.
TIMING OF SEROCONVERSION • IgM – Will be positive in 1-2 weeks after a bite/ECM. Therefore, expect a positive test for early localized (ECM) in only 20-40% of patients. Most sensitive in early disseminated disease stage (neuritis/carditis) -90%+ IgG – tend to convert from 4-6 weeks after bite/ECM.
When Is An IgM WB Helpful ? • Narrow window with early disseminated disease (carditis/neuritis) with no rash hx. High positivity (90%) vs IgG WB (30-40%). • Must reconcile a positive IgM and negative IgG WB in all other clinical presentations where timing does not support serology and assume a FALSE POSITIVE test
IgM WB and “Chronic Lyme” • Recognize that CDC guidelines limit the application of IgM testing to the first month of illness. Misuse/misinterpretation of IgM WB has led to overdiagnosis of Lyme in pts with other illnesses. • When is an exclusive positive IgM WB helpful in cases of chronic complaints – fatigue, myalgias, arthralgias, cognitive ? • EVER ? • NEVER ? • CORRECT ANSWER: NEVER EVER
LYME C6 TESTINGAnother Second Tier TestSteere et al. CID 2008;47:188-95Branda et al. CID 2010;50:20-26 • Another tool in Lyme sero-diagnosis is an IgG ELISA from the C6 region of the variable major protein-like sequence-expressed (VlsE) lipoprotein of B.burgdorferi - Lyme C6. • In prospective studies against two-tier testing, the C6 ELISA proved to have a high sensitivity (100%) of and specificity(96%) in pts with stage 2 or 3 disease. • EM cases only about 30% sensitive with both methods.
LYME C 6 Testingin a 2 Tier IgG-only Approach • Using only C6 test as a second tier test after a positive ELISA screen • C 6 peptide ELISA IgG proved positive earlier in the progression of stages of LD (Stage 2) in 2 independent labs. • This approach eliminates the need for, and confusion with, IgM testing. • As a “stand alone” test, C6 had a lower sensitivity (96%) and specificity (96%) in late LD than 2-tier testing
CAVEATS WITH LYME SEROLOGIES • Early/appropriate antibiotic therapy may often abort a seroconversion. • Background rates of seropositivity in highly endemic areas maybe higher than 5%. • High rates of p23 band positivity (false+) in the general population. • WB are semi-quantitative/subjective –faint bands “+” • Both ELISA and WB (IgM/IgG) positivity may persist for 10-20 years. Subsequent infection can only be made clinically. 79% had + 2-tier testing when asymptomatic as controls in prospective study.
MISUSE OF LYME SEROLOGIES • There is no serologic “test of cure”, so repeated testing after treatment has no prognostic utility- simply adds to patient anxiety, and repeated courses of antibiotics. • There is no marginal change in WB band conversions – ie: declining number of bands to monitor response to treatment.
UTILITY and FUTILITY OF SEROLOGIC TESTING FOR LYME DISEASE • Use serologic studies to support clinical findings of disease stages. • Have a clear understanding of seroconversion timing and rates based on large data bases (IDSA GUIDELINES: CID 2006;43:1089) • Sequential testing may prove useful in evolving cases ie: flu sxs/headache (neg. test) followed by neuritis/carditis/arthritis. • Once serologically positive, future testing for subsequent infections become futile. Must base dx on clinical findings alone. • THERE IS NO TEST OF CURE !
Early Lyme DiseaseTreatment Recommendations Doxycycline or Amoxicillin for 10 to 14 days Erythema Migrans Disseminated skin lesions Early neurologic - cranial neuropathy Parenteral Ceftriaxone for 28 days Early neurologic – meningitis/radiculitis
Late Lyme Disease Treatment Recommendations Doxycycline or Amoxicillin po for 28 days Arthritis Recurrent arthritis (see below) Ceftriaxone 2 gm IV qd Central or peripheral nervous system disease Recurrent arthritis Cardiac disease
Treatment Recommendations Secondary and Late Stage Lyme IV therapy should be reserved for neurologic disease, cardiac involvement or chronic arthritis Do not expect serologies to become negative with treatment. There is no role for sequential testing for cure. There is no data supporting treatment for longer than six weeks. Consequences of prolonged antibiotic therapy include: Development of resistant bacteria C. difficile diarrhea Cholecystitis (Ceftriaxone therapy) Line–associated bacteremia and venous thrombosis.
Single Dose Therapy for Tick Exposure Considered effective therapy to prevent Lyme disease in the following settings: If tick is attached for at least 36 hours - engorged If endemic area If tick bite occurred within 72 hours Doxycycline 200 mg PO x 1 dose
BECOME LYME LITERATEOur Patients Deserve It • Clinical Practice Guidelines by IDSA: Lyme, HGA and Babesiosis CID 2006:43;1089-1134. • Clinical Appraisal of “Chronic Lyme Disease” Feder, et al. NEJM 2007;357: 1422-30. • 2-Tiered Antibody Testing for Early and Late Lyme Disease using IgG Blot with C-6 test> Branda, et al. CID 2010;50:20-26. • Final Report of the Lyme Disease Review Panel of IDSA. Lantos,et al. CID 2010;51:1-5
Anaplasmosis Clinical Features of Infection and Disease
Human Granulocytic AnaplasmosisCellular Pathogenesis Obligate intracellular organisms that replicate within phagosomes of host cells (PMN) and form microcolonies within vacuoles – MORULAE Anaplasma phagocytophilumbinds preferentially to neutrophil surfaces, and monocytes are resistant due to inability to bind/uptake. Once in neutrophils, Anaplasma evades oxidative killing, and inhibits PMN phagocytosis.
Anaplasmosis Trends:New York State and the Capital Region Over the period 2007 through 2011, the number of Anaplasmosis cases reported in NYS rose 1.6 fold, from 205 to 318. Over the same period, the number of cases in the six-county Capital Region rose over 3.6 fold, from 31 to 113. The Capital Region represented only 15% of NYS cases in 2007, but nearly 37% in 2011. The Capital Region accounted for 73% of the total rise in NYS Anaplasmosis cases over this five (5) year period.
Anaplasmosis and Ehrlichiosis Age Distribution of Cases Historically, both Anaplasmosis (HGA) and Ehrlichiosis (HME) have had the highest age-specific incidence in the 60 – 69 and > 70 age groups. Sub-clinical cases most likely exist in the younger age groups, as tick exposures would be more predictable. Infection clears without treatment. Theoretically, the waning immune status of healthy, elderly individuals ( “immunosenescence” ) plays a role in the development of symptomatic disease with both HGA and HME.
Transmission of Anaplasmosis Anaplasmosis may be transmitted via blood transfusion, vertically maternal-child, and by direct contact with a slaughtered deer. A review of nine (9) woman who were diagnosed and successfully treated during pregnancy (rifampin or doxycycline). CID 2007;45:589 A single perinatal transmission to a newborn was confirmed and successfully treated.
Anaplasmosis: Clinical Presentation Fever – otherwise undetermined - 93% Malaise – 94 % Headache - 76 % Myalgias - 77 % Arthralgias – 46 % Nausea (38%), Vomiting (26%), Diarrhea (16%) Rash is Rare – 6 % Yet , in HME – 31 %
Anaplasmosis: Complications Rarely, fulminant cases of untreated Anaplasmosis and HME can occur. Complications may include acute renal failure, respiratory failure and shock. Immunocompromised patients, including HIV, may have a complicated course, especially with HME. Case fatality rates are low. Anaplasmosis - < 1% and HME about 3%.
Anaplasmosis Laboratory Findings and Diagnostic Testing
Anaplasmosis in the Capital Region2007 ( Cases - 31) – 2011 (Cases – 113) Source - NYSDOH
Anaplasmosis Laboratory Features Several very suggestive laboratory findings often bundled Leukopenia Immature neutrophils – Marked left shift Atypical lymphocytes Thrombocytopenia Inverse relationship between mean WBC and platelet count and probability of Anaplasmosis Rise in LFT’s, notably transaminases and LDH
Anaplasmosis Diagnostics Peripheral Blood Smear to search for morulae in neutrophils with sensitivity of 20 – 80% . PCR for both Anaplasmosis and HME with sensitivity of 55 - 87%. Expect a drop in sensitivity > 1 week after illness, and also after treatment onset. Serology – selective IFA of ELISA for Anaplasmosis and HME. Look for a rise in convalescent titer 4 weeks after illness onset.
Anaplasmosis Treatment Doxycycline 100 bid for at least 3 days after defervescence, or 7 – 10 days total. Chloramphenicol is an option. Rifampin for pregnant women. Quinolones have variable in vitro efficacy. American Academy of Pediatrics revised guidelines in 1997 and recommends doxycycline as safe for short-course treatment of tick-borne diseases in children of all ages.
Anaplasmosis Treatment Beta-lactam and macrolide agents have no efficacy against Anaplasmosis or HME. Will see prompt response to treatment in 24 - 48 hrs. Persistent fever would suggest another diagnosis. There is no reported relapse after effective therapy and no syndrome of chronic disease. With objective evidence of concurrent Lyme disease, doxycycline can be trusted to treat both infections (10 - 14 days).
Babesiosis Clinical Features Diagnostic Testing Treatment
BabesiosisClinical Features Similar clinical presentation to malaria, but may range from asymptomatic to fulminant. Most severe in asplenics and immunocompromised. Fevers, chills, sweats Myalgias and arthralgias One-fourth of adults, and one-half of children, may have asymptomatic infection as evidenced by IgG serologies.
BabesiosisLaboratory Features Anemia Often hemolytic anemia Thrombocytopenia Elevated LFT’s NOT the leukopenia and atypical lymphocytosis as evidenced in Anaplasmosis.