Download
1 / 77
770 likes | 1.06k Views
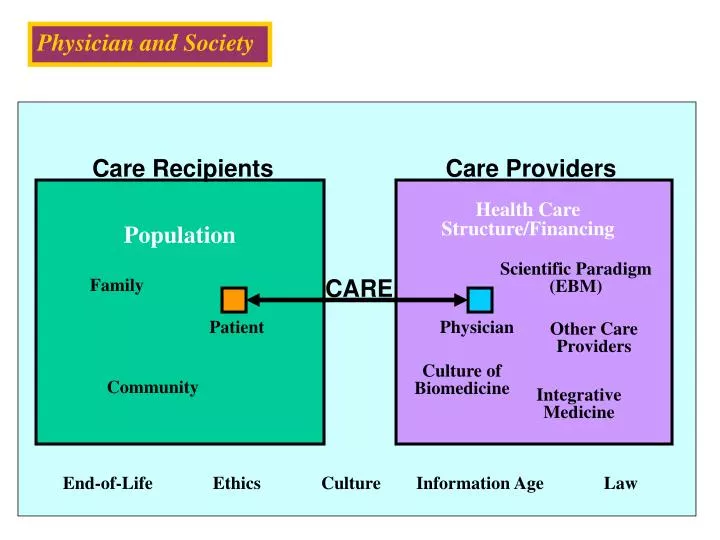
Physician and Society. Physician and Society. Care Recipients. Care Providers. Health Care Structure/Financing. Population. Scientific Paradigm (EBM). Family. CARE. Patient. Physician. Other Care Providers. Culture of Biomedicine. Community. Integrative Medicine. End-of-Life.

E N D
Physician and Society Physician and Society Care Recipients Care Providers Health Care Structure/Financing Population Scientific Paradigm (EBM) Family CARE Patient Physician Other Care Providers Culture of Biomedicine Community Integrative Medicine End-of-Life Ethics Culture Information Age Law
Physician and Society Physician and Society Organizational Strategies Series • 1. Patients, Providers, and Quality • 2. Models of Medical Care • 3. Chronically Ill, Poor, and Uninsured • Use of Informatics in Health Care • Public Health Ethics
Physician and Society Physician and Society Disease Management of Chronic Illness
Physician and Society What is “Disease Management”? • Packaging of familiar and longstanding clinical concepts centered around a condition • Systematic, population-based approach to identify patients at risk, intervene with specific therapeutic programs, and measure clinical outcomes of interest
Physician and Society Proactive Chronic Care (Disease Management) Model Case Finding Assessment Management
Physician and Society Proactive Chronic Care (Disease Management) Model Case Finding Assessment Management
Physician and Society Identifying High-Risk Patients • Recognition by clinicians
Physician and Society Identifying High-Risk Patients • Claims data
Physician and Society Identifying High-Risk Patients • Surveys
Physician and Society Proactive Chronic Care (Disease Management) Model Case Finding Assessment Management
Physician and Society Assessment of High-Risk Patients • Performed by trained CM • Straightforward vs multidimensional needs • Medical and non-medical factors
Physician and Society Proactive Chronic Care (Disease Management) Model Case Finding Assessment Management
Physician and Society Management of High-Risk Patients • Case management • Primary care referral • Specialty care • Team care • Pharmacy • Home care
Physician and Society The Challenge of Chronic Diseases—the Chronic Care Model Ed Wagner MD, MPH MacColl Institute for Healthcare Innovation Group Health Cooperative Improving Chronic Illness Care, a national program of The Robert Wood Johnson Foundation
Physician and Society State of the Art in Chronic Illness Care Improvement • Major clinical advances in most major chronic illnesses • Growing appreciation that the patient’s (and family’s) self-management skill heavily influences outcomes • But, patients not reaping benefits of new knowledge
Physician and Society Current status of Chronic Illness Care in the U.S. • 27% of hypertensives are adequately treated • 29% and 26% of diabetics have well controlled lipid and blood pressure levels, respectively • 35% of eligible patients with atrial fibrillation receive anticoagulation • 25% of people with depression are receiving adequate treatment • 50 % of discharged CHF patients are readmitted within 90 days
Physician and Society Why are we doing so poorly? The IOM Quality Chasm report says: • “The current care systems cannot do the job.” • “Trying harder will not work.”
Physician and Society Usual Chronic Illness Care • Oriented to acute illness • Focus on symptoms and lab results • Patient’s role in management not emphasized • Care dependent on provider’s memory and time • Interaction often not productive, and frustrating for both patient and doctor
Physician and Society What Will Improve Chronic Illness Care? The IOM Quality Chasm report says: • “Changing care systems will.”
Physician and Society The Goal of System Changes to Improve Chronic Illness Care Productive Interactions Practice Team Patient a planned set of interactionsover time during which the critical clinicaland behavioral elements of care are performed reliably
Informed, Activated Patient Physician and Society What characterizes an “informed, activated patient”? They have the motivation, information, skills, and confidence necessary to effectively make decisions about their health and manage it
Physician and Society What characterizes a “prepared” practice team? Prepared Practice Team At the time of encounters, they have the patient information, clinical expertise, team, equipment, and time required to deliver evidence-based clinical management and self-management support
Physician and Society Randomized trials of system change interventions: Diabetes Cochrane Collaborative Review • 41 studies, majority randomized trials • Interventions classified as provider-oriented, organizational, information systems, or patient-oriented • Patient outcomes (e.g., HbA1c, BP, LDL) only improved if patient-oriented interventions included • All 5 studies with interventions in all four domains had positive impacts on patients Renders et al. Diabetes Care 2001;24:1821
Physician and Society Randomized trials of system change interventions: Heart failure • 11 randomized trials • Most reduced hospitalization significantly • Most successful employed a nurse case manager working with cardiology and primary care • Care guided by protocol and strong emphasis on self-management support • 7/8 examining costs found cost savings McAlister et al, Am J Med 2001
Physician and Society Does improved chronic care reduce health care costs? • 28 randomized trials studied interventions related to the chronic care model and examined costs (diabetes, CHF, asthma) • 17 showed either cost savings or utilization decreases Bodenheimer et al. JAMA 2002;288:1909
Physician and Society Interventions Supportive of Productive Interactions • Provider-oriented • Patient-oriented • Practice-orientedInformation Systems
Physician and Society The Goals of System Change Interventions to Improve Practice • Provider-oriented—enable practice team to deliver evidence-based care to EVERY patient • Patient-oriented—develop informed, activated patients who are competent self-managers • Practice-oriented—design practice teams, patient encounters, and data systems that enable productive interactions
Chronic Care Model Community Health System Health Care Organization Resources and Policies ClinicalInformationSystems Self-Management Support DeliverySystem Design Decision Support Prepared, Proactive Practice Team Informed, Activated Patient Productive Interactions Improved Outcomes
Physician and Society Self-management Support Provide effective self-management interventions and ongoing collaborative goal-setting and problem-solving by the team.
Physician and Society Self-management Support What is self-management? “The individual’s ability to manage the symptoms, treatment, physical and social consequences and lifestyle changes inherent in living with a chronic condition.” Barlow et al, person Educ Couns 2002;48:177
Physician and Society Effective self-management Support • patient major role in managing her illnesses and treatment emphasized • her knowledge, behaviors and confidence routinely assessed • goals for improving self-management set collaboratively with practice team • advice based on evidence and presented as information not scolding
Physician and Society Effects of Self-management Education on Glycemic Control • 31 RCTs evaluated effects on HbA1c • Average 6 contacts and 9 contact hours • Most often delivered by nurse-dietician-physician team • 2/3 in groups • Reduction in HbA1c increased with contact time (1% for every added 24 hours of contact) • Effect diminished shortly after end of class Norris et al, Diabetes Care 2002; 25:1159
Physician and Society Delivery System Design • Practice team has defined roles, uses planned visits and clinical case management to support evidence-based care, and assures regular follow-up and care coordination
Nurse Case Management RCT-Aubert et al.Change in Treatment and Glycemic Control Between Baseline and 12 Months
Diabetes Cluster Visits, Sadur et al Change in Treatment and Glycemic Control Between Baseline and 12 Months
Physician and Society Decision Support • Weave evidence-based guidelines into fabric of practice: e.g., reminder and fail-safe systems (e.g., standing orders), specialist involvement with primary care, problem-based learning
Physician and Society ClinicalInformation System: Registry • A database of clinically useful and timely information on all patients provides reminders and feedback and facilitates care planning for individuals or populations
Physician and Society Health Care Organization • Organization encourages and supports better care through leadership, quality improvement& incentives
Physician and Society Community Resources and Policies • Health care organization has linkages with community organizations that can enhance practice capabilities, provide key patient services, or improve care coordination
Physician and Society Examples of Community Linkages • Exercise programs in local Y or gym • Peer support programs • Hospital nurse educator loaned to practice • Endocrine practice nurse loaned
Physician and Society The Quality ChasmUsual Care versusImproved Care • Readmission rates of patients hospitalized with CHF reduced by about 50% • Recovery rates from major depression increased 50-100% • Children with moderately severe asthma have symptoms 14 fewer days/year • Anticoagulated patients in safe and effective range twice as frequently
Physician and Society Differences between Organized Programs and Usual Care of Chronic Illness • Average HbA1c of type II diabetics will be 1%+ lower • 1.5 - 2 times as many patients with major depression will be recovered at six months • Readmission rates of patients hospitalized with CHF will be cut in half • Asthmatic kids will be in school two more weeks a year
BPHC Diabetes Collaboratives 1and 2 involving 180 Community Health Centers and 38,000 diabetic persons Average HbA1c Values
Physician and Society Physician and Society How do you provide care for those who can’t afford it?
Physician and Society Physician and Society Structure and Financing of Care for the Poor and Uninsured in America
Physician and Society Physician and Society Medicaid • Federal/state health insurance program • For low-income persons • 51 million enrollees in 2002 • 2002 Medicaid expenses: $259 billion • 2002 Medicare expenses: $257 billion
Physician and Society Physician and Society Medicaid – Medicare Similarities • Both enacted in 1965 • Both are entitlement programs • Both are overseen by CMS
Physician and Society Medicaid – Medicare Differences • Champion • Medicare: President Johnson • Medicaid: Congress (Wilbur Mills, D-Ark) • Financing • Medicare: purely federal • Medicaid: joint federal/state
Physician and Society Medicaid – Medicare Differences • Beneficiaries • Medicare: Virtually all elderly • Medicaid: All ages • Covered Benefits • Medicare: set by feds, same for all enrollees • Medicaid: set by states, different by states
Physician and Society Medicaid – Medicare Differences • Enrollment Criteria • Medicare: age and/or disability only; set by feds • Medicaid: financial and other health and social criteria; set by individual states