Download
1 / 1
10 likes | 108 Views
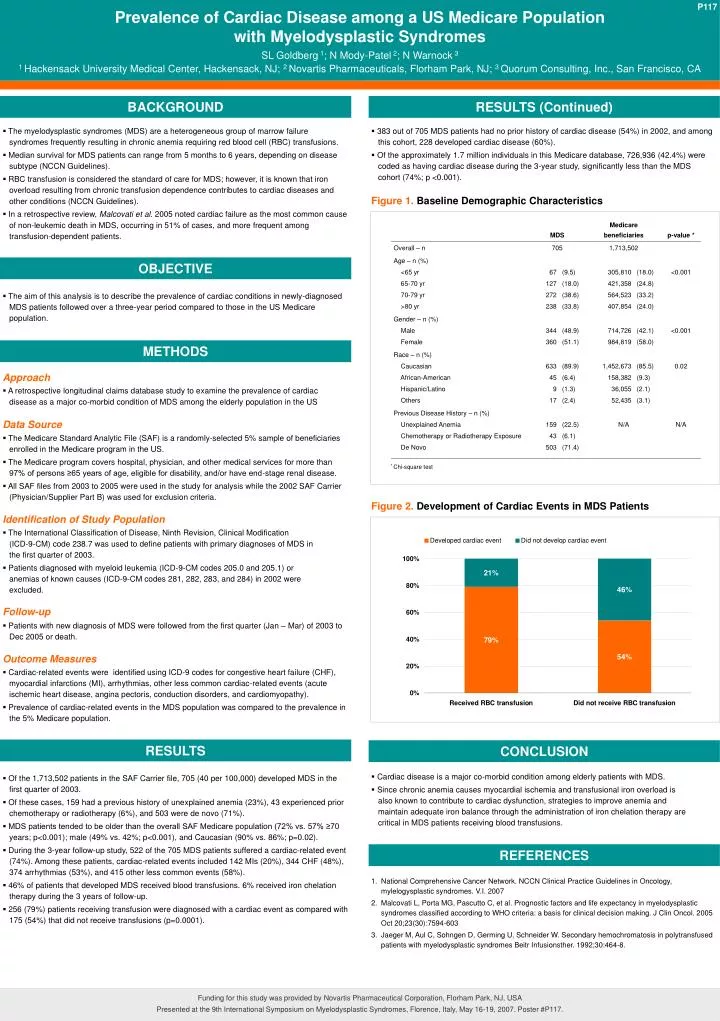
P117. P117. Prevalence of Cardiac Disease among a US Medicare Population with Myelodysplastic Syndromes. SL Goldberg 1 ; N Mody-Patel 2 ; N Warnock 3

E N D
P117 P117 Prevalence of Cardiac Disease among a US Medicare Population with Myelodysplastic Syndromes SL Goldberg 1; N Mody-Patel 2; N Warnock 3 1 Hackensack University Medical Center, Hackensack, NJ; 2 Novartis Pharmaceuticals, Florham Park, NJ; 3 Quorum Consulting, Inc., San Francisco, CA BACKGROUND RESULTS (Continued) • The myelodysplastic syndromes (MDS) are a heterogeneous group of marrow failure syndromes frequently resulting in chronic anemia requiring red blood cell (RBC) transfusions. • Median survival for MDS patients can range from 5 months to 6 years, depending on disease subtype (NCCN Guidelines). • RBC transfusion is considered the standard of care for MDS; however, it is known that iron overload resulting from chronic transfusion dependence contributes to cardiac diseases and other conditions (NCCN Guidelines). • In a retrospective review, Malcovati et al. 2005 noted cardiac failure as the most common cause of non-leukemic death in MDS, occurring in 51% of cases, and more frequent among transfusion-dependent patients. • 383 out of 705 MDS patients had no prior history of cardiac disease (54%) in 2002, and among this cohort, 228 developed cardiac disease (60%). • Of the approximately 1.7 million individuals in this Medicare database, 726,936 (42.4%) were coded as having cardiac disease during the 3-year study, significantly less than the MDS cohort (74%; p <0.001). Figure 1. Baseline Demographic Characteristics OBJECTIVE • The aim of this analysis is to describe the prevalence of cardiac conditions in newly-diagnosed MDS patients followed over a three-year period compared to those in the US Medicare population. METHODS Approach • A retrospective longitudinal claims database study to examine the prevalence of cardiac disease as a major co-morbid condition of MDS among the elderly population in the US Data Source • The Medicare Standard Analytic File (SAF) is a randomly-selected 5% sample of beneficiaries enrolled in the Medicare program in the US. • The Medicare program covers hospital, physician, and other medical services for more than 97% of persons ≥65 years of age, eligible for disability, and/or have end-stage renal disease. • All SAF files from 2003 to 2005 were used in the study for analysis while the 2002 SAF Carrier (Physician/Supplier Part B) was used for exclusion criteria. * Chi-square test Figure 2. Development of Cardiac Events in MDS Patients Identification of Study Population • The International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) code 238.7 was used to define patients with primary diagnoses of MDS in the first quarter of 2003. • Patients diagnosed with myeloid leukemia (ICD-9-CM codes 205.0 and 205.1) or anemias of known causes (ICD-9-CM codes 281, 282, 283, and 284) in 2002 were excluded. Follow-up • Patients with new diagnosis of MDS were followed from the first quarter (Jan – Mar) of 2003 to Dec 2005 or death. Outcome Measures • Cardiac-related events were identified using ICD-9 codes for congestive heart failure (CHF), myocardial infarctions (MI), arrhythmias, other less common cardiac-related events (acute ischemic heart disease, angina pectoris, conduction disorders, and cardiomyopathy). • Prevalence of cardiac-related events in the MDS population was compared to the prevalence in the 5% Medicare population. RESULTS CONCLUSION • Cardiac disease is a major co-morbid condition among elderly patients with MDS. • Since chronic anemia causes myocardial ischemia and transfusional iron overload is also known to contribute to cardiac dysfunction, strategies to improve anemia and maintain adequate iron balance through the administration of iron chelation therapy are critical in MDS patients receiving blood transfusions. • Of the 1,713,502 patients in the SAF Carrier file, 705 (40 per 100,000) developed MDS in the first quarter of 2003. • Of these cases, 159 had a previous history of unexplained anemia (23%), 43 experienced prior chemotherapy or radiotherapy (6%), and 503 were de novo (71%). • MDS patients tended to be older than the overall SAF Medicare population (72% vs. 57% ≥70 years; p<0.001); male (49% vs. 42%; p<0.001), and Caucasian (90% vs. 86%; p=0.02). • During the 3-year follow-up study, 522 of the 705 MDS patients suffered a cardiac-related event (74%). Among these patients, cardiac-related events included 142 MIs (20%), 344 CHF (48%), 374 arrhythmias (53%), and 415 other less common events (58%). • 46% of patients that developed MDS received blood transfusions. 6% received iron chelation therapy during the 3 years of follow-up. • 256 (79%) patients receiving transfusion were diagnosed with a cardiac event as compared with 175 (54%) that did not receive transfusions (p=0.0001). REFERENCES National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology, mylelogysplastic syndromes. V.I. 2007 Malcovati L, Porta MG, Pascutto C, et al. Prognostic factors and life expectancy in myelodysplastic syndromes classified according to WHO criteria: a basis for clinical decision making. J Clin Oncol. 2005 Oct 20;23(30):7594-603 Jaeger M, Aul C, Sohngen D, Germing U, Schneider W. Secondary hemochromatosis in polytransfused patients with myelodysplastic syndromes Beitr Infusionsther. 1992;30:464-8. Funding for this study was provided by Novartis Pharmaceutical Corporation, Florham Park, NJ, USA Presented at the 9th International Symposium on Myelodysplastic Syndromes, Florence, Italy, May 16-19, 2007. Poster #P117.