Download
1 / 35
370 likes | 935 Views
Localising the lesion: “where in the CNS”. Kate Hassan. Learning objectives. Definition of CNS and PNS Definition of UMN and LMN Function of each of the cerebral lobes The homunculus Circle of willis and blood supply to the cerebral hemispheres Motor tracts – lateral corticospinal

E N D
Localising the lesion: “where in the CNS” Kate Hassan
Learning objectives • Definition of CNS and PNS • Definition of UMN and LMN • Function of each of the cerebral lobes • The homunculus • Circle of willis and blood supply to the cerebral hemispheres • Motor tracts – lateral corticospinal • Sensory tracts – lateral spinothalamic and dorsal columns • Stroke syndromes • Clinical case scenarios
Definitions • CNS = Brain and spinal cord • PNS = anything outside brain and spinal cord • Also include autonomic nervous system and cranial nerves
Motor control systems • Corticospinal (pyradmial) • Skilled, intricate, strong and organised movements • Defectiveness loss of skilled voluntary movement, spasticity and reflex changes • Extrapyradimal system • Fast, fluid movements that the corticospinal system has generated • Defectiveness bradykinesia, rigidity, tremor, chorea • The cerebellum • Co-ordinating smooth and learned movement initiated by the pyradimal system and in posture and balance control • Defectiveness ataxia, past pointing, action tremor and incoordination
Sensory pathways • Peripheral nerves carry sensation from dorsal roots to the cord • Posterior columns (dorsal columns) • Vibration, joint position, light touch and point discrimination • Cross in the brainstem passing to the thalamus • Spinothalamic tracts • Pain and temperature • Cross within the cord and pass in the spinothalamic tracts to the thalamus and reticular formation • Sensory cortex • Fibres from the thalamus pass to the parietal region sensory cortex and motor cortex
Cortical functions • Frontal lobe • Reasoning, planning, parts of speech, movement, emotions and problem solving • Left frontal = broccas area (aphasia) • Parietal lobe • Movement, orientation, recognition, perception of stimuli • Occipital lobe • Visual processing • Temporal lobe • Perception and recognition of auditory stimuli, memory and speech • Left temporal = wernicke’s area • Cerebellum • Balance and co-ordination • Basal ganglia • Initiation and inhibition of movement
quiz • Patient has difficulty walking and slurred speech • Cerebellum • Patients wife reported personality change and difficulty wording what they wanted to say • Frontal lobe • Patient has difficulty recognising objects and often gets lost unable to find their way home • Parietal and occipital lobe • Patient has difficulty remembering significant past events and no longer enjoys listening to music • Temporal lobe
Stroke syndromes • TACS = total anterior circulation syndrome • PACS = partial anterior circulation syndrome • POCS = posterior circulation syndrome • LACS = lacunar syndrome
Stroke • TACS – All three of • Hemiplegia or hemi sensory loss • Visual field defect • Disturbance of higher function • Dysphasia • Dysphagia • PACS – 2 out of 3 • LACS – blockage of small branch of big artery • No visual field defect • Pure motor stroke • Pure sensory • Sensory motor • Ataxia • POCS – brain stem, cerebellum, cranial nerves • Bilateral motor or sensory • Conjugate eye movement disorder • Cerebeller dysfunction • Hemiplegia or cortical blindness
Stroke • Acute occlusion of blood vessel leading to hypoxia and infarction • Risk factors • DM, hypertension, smoking, hypercholesterolemia, FHx, AF • Investigations • bloods, CT, MRI, carotid dopplers, Echo, ECG, 24 hour tape • Treatment in ischaemic stroke • Aspirin • Clopidogrel • Supportive management
Cerebellar syndrome • Causes • Vascular lesion • Alcohol • Demyelination • Tumours • Hypothyroidism • Metabolic disorders • Signs “DANISH” • Dysdiadochokinesis • Ataxia • Nystagmus • Intention tremor • Slurred speech, dysarthria • Hpyotonia, hyporeflexia
Multiple Sclerosis • Areas of demyelination and perivascular inflammation (white plaques) • Disseminated in time and occurring anywhere within CNS • Aetiology - ?autoimmune ?vitamin D deficiency • Classification • Benign • Relapse remitting • Secondary chronic progressive • Primary progressive • Investigations • LP – increased protein, increased immunoglobulin, oligoclonal bands • Visual evoked potentials • MRI
Multiple sclerosis • On examination • Unsteady gait • Reduced proprioception • Brisk reflexes • Brown-sequard syndrome • Loss of movement on same side as damage • Loss of pain and temp and sensation on opposite side • Management • Symptoms control (tremors, pain, muscle spasms) • steroids • Beta-inferons • Glatiramer • IV natalizumab
Motor neurone disease • Degeneration of upper and lower motor neurones of unknown cause • 5-10% autosomal dominant • Types • Spinal muscular atrophy – limb weakness due to involvement of spinal cord anterior horn cells • Primary later sclerosis – spastic limb weakness due to UMN involvement of the spinal cord • Progressive bulbar palsy – involvement of bulbar motor neurones, progressive disease • Amyotrophic lateral sclerosis – mixture of all the above • Investigations • Diagnosed clinically after other causes excluded • EMG confirms fasciculation's and fibrillations • Management – symptom control • Fatal within 3-5 years
Motor neurone disease • Cardiac and smooth muscle aren’t involved and ocular muscle very rarely • Autonomic dysfunction occurs late • Signs • Dysarthria, brisk jaw reflex • Fasciculation/wasting in deltoids, biceps, quadriceps and in tongue • Weakness in all4 limbs, brisk reflexes in arms, absent in legs • Combination of UMN and LMN
Clinical case 1 • 23, female presents to her GP with a 2 week history of bilateral leg weakness having started with pins and needles and numbness in her hands and feet. She has had a few days of urinary incontinence which has resolved. 2 years ago she had an episode of blurred vision and pain in the right eye which lasted a month and fully resolved
Case 1 • What is the most likely diagnosis? • What other signs or symptoms might you see in this condition? • What is the pathological basis of this disorder? • What further investigations would you do? • How would you manage this patient?
Clinical case 2 • 61 female • Becoming increasingly weak on her right side over a one week period. She is unable to walk and has slurred speech and right side of her face is drooping • Past history of breast cancer • o/e – right facial weakness, grade 4/5 weakness of the right arm and leg, right homonymous hemianopia and some difficulty naming objects and reflexes are brisk on the right side and her right plantar response is upgoing
Case 2 • What is the likely diagnosis?
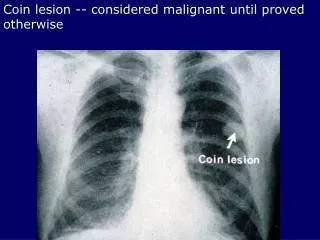
Case 2 • CT head shows extensive oedema surrounding the subtle impression of a ring enhanced lesion in the left frontal lobe, extending into the left parietal lobe. There is associated mass effect displacing the lateral ventricle
Case 2 • What is the likely cause? • Other features that may be present? • What management options are available?
Case 3 • 76 male • Background of AF (on warfarin) has 2 hour history of severe global right sided weakness. He is eye-opening to painful stimuli and is moving his left side spontaneously. When questioned he seems confused
Case 3 • What is his GCS? • What is the diagnosis? • What investigations would you do? • What are the important risk factors? • How wound you manage this patient?
Case 4 • 56 male • 6 month history of progressive weakness of his right hand. Also had problems with swallowing and has choked whilst eating on several occasions • o/e he has wasting of his upper and lower limbs and some fasciculation's were noted his right plantar was up going and his reflexes were generally brisk
Case 4 • Diagnosis? • What investigations would you perform? • How would you manage this patient?
Thank you for listening Any questions?