Download
1 / 31
320 likes | 385 Views
Learn about the incidence, risk factors, diagnosis, treatment, recurrences, and advanced treatment options for metastatic melanoma. Discover the role of BRAF mutations and available therapies like immunotherapy and targeted treatments. Stay informed on clinical trials and advancements in the field.

E N D
Modern therapy in oncology – metastatic melanoma Łukasz Kwinta
Melanoma • Melanoma (malignant melanoma) – malignant neoplasm of the skin, mucosa or uvea derived from melanocytes
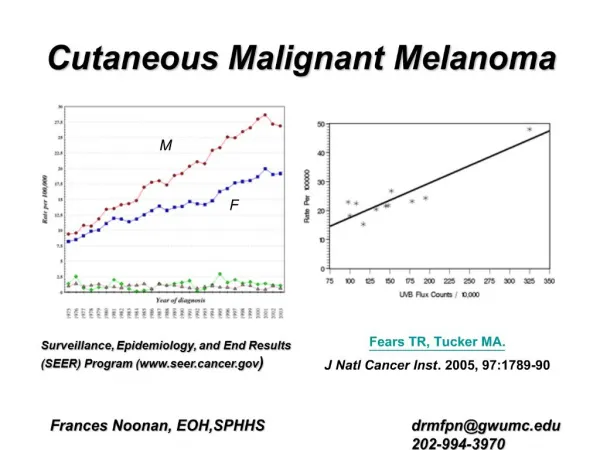
Skin melanoma - incidence • The incidence of melanoma in Poland (2010): almost 1,200 in men and 1,350 in women • Annuallymore than 100,000 cases worldwide. • Melanoma represents 1% of malignant tumors and 5-7% of skin cancers • The growing trend of skin melanoma incidence in both sexes – 3-fold increase over three decades • Geografical differences in incidence • Globally 2,4 – 3,1/100,000 • South-central Asia 0,2/100,000 • Australia 37/100000 (Queensland 43-56/100,000)
Melanoma in USA (Surveillance, Epidemiology and End Results Program)
Risk factors • Exposure to UV radiation (sun, artificial source of radiation) • Intensive intermittent exposure to UV (especially sunburns during chilhood) is linked to higher risk than long-term regular exposure • Sunbeds • Family history of melanoma (10%) • Dysplastic nevus syndrome • Immunosuppression
Diagnosis: Physical examination – examination of WHOLE skin, including „problematic” areas (hairy skin of the head, feet, interdigital spaces, genital and anal areas) Dermatoscopy and videodermatoscopy
Diagnosis of skin melanoma: Histopatologic examination of whole primary lesion (excisional biopsy) – no neddle biopsy!!!
Treatment: Depends on: -depth of invasion (Breslow) -ulceration -mitotic activity (number of mitosis/mm2) -lymph nodes involvement -distant metastases
Sentinel lymph node biopsy (excision) • Sentinel node is the first lymph node in the way of lymphatic drainage • Sentinel node is usually the first location of lymphatic metastases • The absence of metastases in the sentinel node does not allow to exclude the presence of nodal and distant metastases (can develop as a result of blood spread)
Regional lymph nodes excision • It has been shown that involvement of the sentinel node is associated with approximately 18% risk of involvement ofother regional lymph nodes • Regional lymph node dissection (lymphadenectomy) improves local control of disease and reduce the risk of distant metastases • Removal of all possible lymph nodesdraining lymph from region involved by primaty lesion
Types of recurrences • Local recurrence • Satellite and in transit lesions • Nodal recurrence • Distant organs metastates
Advanced and disseminated melanoma - treatment Qualification for further treatment by a multidisciplinary therapeutic teams Consider qualification for clinical trials Determination of BRAF V600 mutation (in metastatic or primary lesions Available therapies: CTLA-4 inhibitors (ipilimumab), PD-1 inhibitors (pembrolizumab, nivolumab), BRAF inhibitors (vemurafenib, dabrafenib) in combination with MEK inhibitors (cobimetinib, trametinib), IL2, chemotherapy, radiotherapy, surgery, T-VEC.
BRAF V600 activating mutation • BRAF kinase is a serine-threonine kinase activating MEK/ERK kinases • The gene is classified as protooncogene • Activating mutation (oncogene) is a relatively frequently present in many types of cancer. • Mutated BRAF gene is involved in the pathogenesis of melanoma by constitutive activation of MEK/ERK pathway (impact on potential for replication, angiogenesis, ability to infiltrate tissues and to metastasize, avoiding immune response and apoptosis) • BRAF mutation leads to uncontrolled tumor cell proliferation
SYSTEMIC TREATMENT IN BRAF-MUTATED MELANOMA - Targeted therapies (preferred when fast response is needed – risk of visceral crisis) Vemurafenib Dabrafenib Dabrafenib+Trametinib Wemurafenib+Cobimetinib - Immunotherapy Nivolumab Pembrolizumab - Clinical trials
Immunotherapy The hypothesis of immune surveillance was established in the 60s and 70s by Sir Frank Burnet Macfarlance The human immune system is constantly searching and eliminating tumor cells Progress in the understanding of the functioning of the immune system has enabled a detailed definition of immune mechanisms eliminating cancer cells Development of immunooncology
Immunotherapy Median survival of metastatic melanoma before 2011 (before approvals of immunoterapies/targeted therapies) - 6-9 months Immunological check-points inhibitors CTLA-4 inhibitor Ipilimumab(Yervoy) PD-1 inhibitor Nivolumab(Opdivo) Pembrolizumab (Keytruda)
Metastatic melanoma – additional possibilities of treatment - Chemotherapy DTIC, temozolomide, paclitaxel, fotemustine, multi-drugs regimens - Surgery radical resections of single metastasis in patients in good permormance status - Radiotherapy metastatic lesions of CNS, painful metastases in bones or other organs