Download
1 / 32
330 likes | 514 Views
Measuring Action Potential Conduction Velocity and Determining the Site and Extent of Spinal Cord Injuries based on Sensory Deficits. The proximity of the Ulnar nerve near the surface at elbow and wrist makes it well suited for studying action potential conduction velocity.

E N D
Measuring Action Potential Conduction VelocityandDetermining the Site and Extent of Spinal Cord Injuries based on Sensory Deficits
The proximity of the Ulnar nerve near the surface at elbow and wrist makes it well suited for studying action potential conduction velocity.
The ulnar nerve has both efferent (motor) and afferent (sensory) axons.
Stimulating the ulnar nerve at the elbow or wrist will produce sensations and contractions of muscles in the hand. What types of sensory axons are in the ulnar nerve and what will you feel when action potentials are induced in those axons?
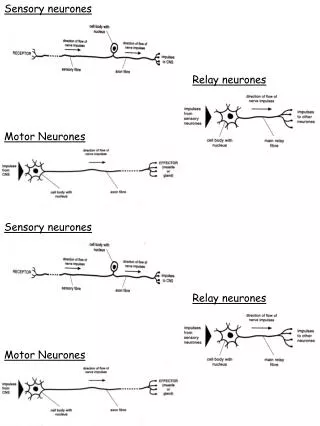
Neuromuscular Junctions (NMJs) and Synaptic Delay Action potentials in efferent axons arrive at NMJ Release of neurotransmitter (Acetylcholine)Depolarization of muscle cell membraneAppearance of action potential in muscle cellsMuscle contraction
Choir = a muscle consisting of individual muscle cells (each singer) Choir output = sum of individual voices Electromyogram = sum of action potentials for all active muscle cells Single stimulus (command from conductor) produces Compound Muscle Action Potential
Peripheral nerve with afferent and efferent axons The Neuromuscular Junction andSynaptic Delay Cars = action potentials conducted along axons (lanes) Distance1/time1 Distance2/time2 Distance1-Distance2-/time1-time2 = highway speed = conduction velocity in axons!
An excellent resource on discriminating between the various causes of muscle weakness demonstrating the diagnostic power of transcutaneous electrical stimulation and recording compound muscle action potentials. Website Remember to measure the two distances!
+ or - Groundon dorsumof hand
Exit Scope software.Load LabChart software, then exit.Reload Scope program. PowerLab Scope 4.1 Settings: Input B = Off, Input A = Ch 3, BioAmp range 10 mV or 5 mV or as necessary to see Compound Muscle Action Potential Timebase = 50 msSamples = 2560 (40KHz) Setup/ Stimulator: Check Isolated, mode = pulse, delay = 10 ms, duration = 200 us, Amplitude = 20 mA. Display: Overlay stimulator to Input A, Set up: Sampling = Sweep= Multiple, 32 sweepsSource= User, 0.5 sec delay, Display/Overlay All. To examine individual recording, select Display/Overlay None. Use M (Marker) to measure times. Measure latency from stimulus to first positive or negative peak of Compound Muscle Action Potential from Wrist and from Elbow.
Which arm to test is determined randomly by last digit of SSN: • Even number test Right Arm • Odd number test Left Arm. Enter your data into the Spreadsheet on the Side Bench Computer
This paper describes the various clinical applications of the techniquewere using today! Could be a useful reference for some abstracts. Role of Neurophysiologic Evaluation in Diagnosis Journal of the American Academy of Orthopaedic Surgeons May/June 200 Vol 8 No. 3 p 190-199 Lawrence R. Robinson, MD Dr. Robinson is Professor of Rehabilitation Medicine, University of Washington School of Medicine, Seattle, and Chief of Rehabilitation Medicine and Director, Electrodiagnostic Medicine Laboratory, Harborview Medical Center, Seattle. Reprint requests: Dr. Robinson, Rehabilitation Medicine, Harborview Medical Center, Box 359740, 325 Ninth Avenue, Seattle, WA 98104. Abstract The electrodiagnostic evaluation assesses the integrity of the lower-motor-neuron unit (i.e., peripheral nerves, neuromuscular junction, and muscle). Sensory- and motor-nerve conduction studies measure compound action potentials from nerve or muscle and are useful for assessing possible axon loss and/or demyelination. Needle electromyography measures electrical activity directly from muscle and provides information about the integrity of the motor unit; it can be used to detect loss of axons (denervation) as well as reinnervation. The electrodiagnostic examination is a useful tool for first detecting abnormalities and then distinguishing problems that affect the peripheral nervous system. In evaluating the patient with extremity trauma, it can differentiate neurapraxia from axonal transection and can be helpful in following the clinical course. In patients with complex physical findings, it is a useful adjunct that can help discriminate motor neuron disease from polyneuropathy or myeloradiculopathy due to spondylosis. Link to the abstract.
How are stimuli delivered to one side of the body processed on the opposite (contralateral) side of the brain? Right side Left side Right side Left side source
Left side of brain Right side of body Left side of body
Diagnosis the level and extent of spinal cord injury based on sensory deficits. Source
For simplicity, all our cases will involve injury either at high cervical levels (which produce sensory deficits in hands and feet) or mid-thoracic levels (which do not affect hands.)
Case # 4 All sensations normal except loss of pain and temperature from the right foot.
Body-sense sensations • Proprioceptorsare receptors that give information about body position. • These receptors are located in muscles, tendons, ligaments, joints and skin. • Somesthetic sensations (senses associated with the surface of the body). • Mechanoreceptors detect pressure, force and vibration. These include: • Merkel's disks and Meissner's corpuscles in the superficial layer of the skin and, hair follicle receptors, Pacinian corpuscles and Ruffini's endings in deeper layers. • Thermoreceptors respond to temperature of receptor endings themselves. • Warm receptors respond to temperature between 30oC and 45o C with action potentials increasing as temperature increases. • Cold receptors respond to temperatures between 35o C and 20o C with action potentials increasing as the temperature falls. Both warm and cold receptors respond rapidly to temperature changes and show rapid adaptation. The brain uses the relative changes in the responses of hot and cold receptors to interpret the temperature of the environment. • Nociceptorstransduce harmful stimuli that we perceive as pain. These consist of free nerve endings. There are three types of nociceptors: • Mechanical - respond to intense mechanical stimuli. • Thermal - respond to intense heat. • Polymodal - respond to a variety of stimuli including mechanical, intense heat and chemicals released from damaged tissue.