Download
1 / 31
310 likes | 500 Views
Clarithromycin Subject 4003/3212/003 with ERSP Isolates, PPb. Presentation : 51 year old female, Fine Score II, no relevant risk factors for pneumonia Chest X-ray : Right median lobe pneumonia and right inferior lobe Blood cultures :

E N D
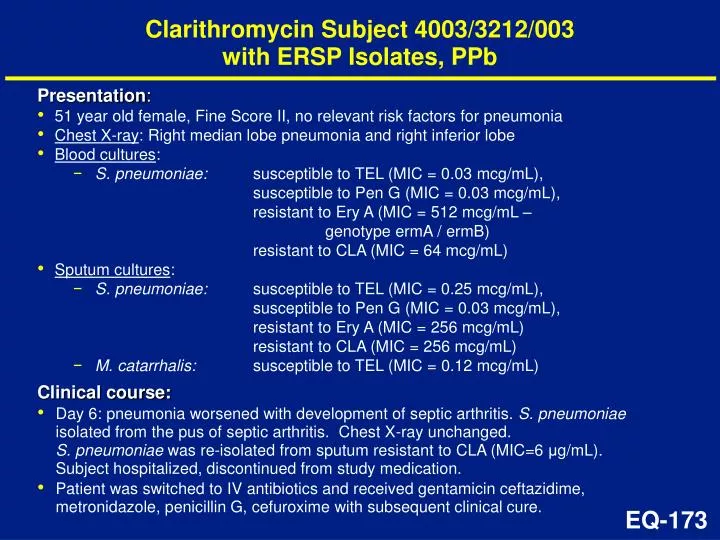
Clarithromycin Subject 4003/3212/003with ERSP Isolates, PPb • Presentation: • 51 year old female, Fine Score II, no relevant risk factors for pneumonia • Chest X-ray: Right median lobe pneumonia and right inferior lobe • Blood cultures: • S. pneumoniae: susceptible to TEL (MIC = 0.03 mcg/mL),susceptible to Pen G (MIC = 0.03 mcg/mL),resistant to Ery A (MIC = 512 mcg/mL – genotype ermA / ermB) resistant to CLA (MIC = 64 mcg/mL) • Sputum cultures: • S. pneumoniae: susceptible to TEL (MIC = 0.25 mcg/mL),susceptible to Pen G (MIC = 0.03 mcg/mL),resistant to Ery A (MIC = 256 mcg/mL) resistant to CLA (MIC = 256 mcg/mL) • M. catarrhalis: susceptible to TEL (MIC = 0.12 mcg/mL) • Clinical course: • Day 6: pneumonia worsened with development of septic arthritis. S. pneumoniae isolated from the pus of septic arthritis. Chest X-ray unchanged. S. pneumoniae was re-isolated from sputum resistant to CLA (MIC=6 μg/mL). Subject hospitalized, discontinued from study medication. • Patient was switched to IV antibiotics and received gentamicin ceftazidime, metronidazole, penicillin G, cefuroxime with subsequent clinical cure.
All CAP Studies (Pooled): Key Demographics, mITT TEL COMP 5 d 7–10 d 7–10 d N=187 N=2102 N=702 Sex Male 118 (63%) 1172 (56%) 357 (51%) Female 69 (37%) 930 (44%) 345 (49%) Age Mean 45.4 44.7 45.6 (yrs) 13–18 1 (1%) 51 (2%) 21 (3%) 18 – 65 156 (83%) 1748 (83%) 557 (79%) 65 30 (16%) 303 (14%) 124 (18%) Race White 134 (72%) 1427 (68%) 544 (78%) Black 34 (18%) 504 (24%) 123 (18%) Asian 5 (3%) 28 (1%) 8 (1%) Other 14 (8%) 142 (7%) 26 (4%)
Post-Marketing Reports of Symptomatic Liver Injury : 200214202DE (1) • 70 M with history of COPD, Billroth II stomach resection, hepatitis A, diabetes • medications: prednisolone, fenoterol/ipratropium, formoterol, theophylline, ursodeoxycholic acid, cholestyramine, lactulose, acetylcysteine, • Treated with TEL for AECB and flu-like illness • Day 14: admitted to hospital for recurrent AECB • treated with high dose corticosteroids and AMC during 3-week hospitalization • Day 27: discharged home HK-136
Post-Marketing Reports of Symptomatic Liver Injury : 200214202DE (2) • Day 50: readmitted with cholestatic hepatitis with jaundice • peak ALT 132 U/l, AP 735 U/l, TB 25 mg/dl • Day 51: Ultrasound: homogeneous liver with 2mm (enlarged) common bile duct, gall bladder polyps • Day 58: Liver biospy: marked cholestasis with mononuclear cell infiltrate, singular cell necrosis with surrounding granulocyte reaction • interpreted as consistent with drug-induced cholestatic hepatitis • Full recovery after ~ 3 months HK-137
Post-Marketing Reports of Symptomatic Liver Injury : 200213635DE • 33 F with no significant medical history • medications: ethinylestradiol-levonorgestrol for 3 years • Treated with TEL x 5 days for bronchitis/sinusitis • Day 3: Elevation of transaminases • ALT 388, AP normal, TB 33 (ULN <21) • symptoms: nausea, vomiting, RUQ pain, fever, asthenia • normal eosinophils • Full recovery noted after 5 weeks HK-139
Post-Marketing Reports of Symptomatic Liver Injury : 200211855DE • 44 F with history of COPD • medications: budesonide, beta-agonist inhaler, coritcosteroids • Treated with TEL x 10 days for febrile infection • Day 2: Onset of fatigue, right upper quadrant pain • Day 3: hospitalized • transaminases in 2-300 range (no values provided), alkaline phosphatase 800U/l, normal bilirubin • autoimmune and viral serology negative • ultrasound normal • Full recovery noted in 15 days HK-141
Post-Marketing Reports of Symptomatic Liver Injury : 200211440DE • 61 F with history of recurrent endocarditis • medications: acetyldigoxin • Treated with TEL x ~ 10 days for Sinusitis/tonsillitis • ~ Day 14: Limited effect with relapse of fever • hospitalized for suspected endocardititis; work-up negative • Had LFT , hepatic labs and work-up (eg viral serology and other infectious causes) not provided • Discharged with improvement • Biopsy performed several days after discharge: • focal fatty degeneration (mixed vacuole size) with moderate intrahepatic cholestasis; mild inflammatory (lymphocyte) infiltrate; no eosinophils • Interpreted as nutritive-toxic origin • Reporting Physician felt overall course not suggestive of drug-induced etiology HK-142
B. fragilis 0.03 - >128 Bacteroides spp. 0.03 - >64 Prevotella spp. 0.01 - 8.0 Porphyromonas spp. 0.001 - >32 Fusobacterium spp. 0.015 ->64 Actinomyces spp. <0.015 Peptostreptococcus spp. <0.008 - 16 Propionibacterium spp. <0.015 - 0.03 Clostridium spp. <0.008 - 0.25 C. difficile 0.06 - >64 Telithromycin: Anaerobes – MIC Ranges (μg/mL) MI-38
Telithromycin Subject 3000/605/1091 • Presentation: • 78 year old female, Fine score III • Chest X-ray: consolidation • Blood cultures: • S. pneumoniae: susceptible to TEL (MIC = 0.03 mcg/mL),susceptible to Pen G (MIC = 2 mcg/mL),resistant to Ery A (MIC = 32 mcg/mL) – genotype ermB • Respiratory cultures: H. influenzae: susceptible to TEL (MIC = 1 mcg/mL) M. catarrhalis: TEL MIC not performed, susceptible by disk • Clinical course: • Initial improvement and sterilization of blood culture at day 12 of therapy, subject had a recurrence of dyspnea and fever associated with a secondary UTI (S. aureus), treated with intravenous antibiotics • Clinical status at TOC was improved, blood culture negative for S. pneumoniae (presumed persistent because of the IV antibiotic) EQ-146
QTc vs Telithromycin Plasma Concentration in Phase III Studies Concs 5µg/mL Conc QTc QTc 5.2 410 -7.4 5.2 364 -24.5 5.2 411 13.1 5.2 409 -3.3 5.3 428 -0.9 5.8 431 17.0 6.2 425 1.5 6.2 410 10.1 6.4 391 -38.8 6.4 381 -5.1 6.4 393 -6.0 6.7 435 18.0 7.2 408 17.8 7.8 396 0.1 9.9 427 8.7 120 80 40 0 QTc (ms) -40 -80 N=1512 patients Slope=0.88 ms/µg/mL r2=0.0025, p0.05 -120 -160 0 2 4 6 8 10 12 Concentration (µg/mL) CK-12
Study 3014: Usual Care (24,000 subjects comparative study) • Large experience of co-morbidities (e.g. elderly, elderly female, CHF, CAD) known to increase TdP risk without any clinical signal (death, arrhythmic death, syncope). • Large experience of co-therapies (e.g. CYP P450 inhibitors, diuretics, drugs prolonging QTc, digitalis, antiarrhythmics, ) known to increase TdP risk without any clinical signal (death, arrhythmic death, syncope). • Absence of mortality, arrhythmic death or syncope signals in real-use trial vs. AMC • Time-course of arrhythmic deaths mitigates against any causal relationship (occurred more than 7 days after telithromycin therapy completed). CK-13
Study 3014: Cardiac AESIs in Subjects at Risk of TdP (1) No. of subjects with cardiac AESIs Co-morbidities TEL AMC 65 years 21/2273 (0.9) 21/2203 (1.0) Women 65 years 10/1235 (0.8) 10/1204 (0.8) 75 years 10/892 (1.1) 11/873 (1.3) CHF 5/277 (1.8) 3/271 (1.1) CAD 15/837 (1.8) 10/872 (1.1) TEL = telithromycin, AMC = amoxicillin-clavulanic acid CK-16
Study 3014: Cardiac AESIs in Subjects at Risk of TdP (2) No. of subjects with cardiac AESIs Co-therapies TEL AMC Diuretics 13/1776 (0.7) 12/1710 (0.7) Drugs prolonging QTc* 11/1974 (0.6) 10/1906 (0.5) Digitalis 2/20 (1.0) 4/230 (1.7) CYP3A4 inhibitors 4/2309 (0.2) 11/2201 (0.5) *Includes anti-arrhythmics TEL = telithromycin, AMC = amoxicillin-clavulanic acid CK-17
Subject 200214256DE: Spontaneous Report: Fatal Ventricular Arrhythmia (1) • 59 y/o male treated with TEL for acute sinusitis • Med Hx: coronary heart failure, angina pectoris, HTN, cardiac stent 2x, triglycerides/cholesterol, manic depressive, spastic paraplegia, obesity (130 kg), daytime somnolence • Family Hx: sudden death, brothers (48 yr, 49 yr), mother (59 yr) • Con Meds: triamterene, baclofen, isosorbide, diazepam, metoprolol, amlodipine, mirtazipine, atorvastatin CK-26
Subject 200214256DE: Spontaneous Report: Fatal Ventricular Arrhythmia (2) • 3 Days pretreatment: syncopal episode preceded by pallor, incoherent speech • Day 6: confusion, normal ECG & BP, neuro exam normal • Day 9: motor vehicle accident from possible syncope and hospitalized; resolved at admission Labs: K+ 3.6 mmol/L; ECG: NSR, 60 bpm, normal QTc • Day 10: patient found dead at 16.30 14:57: NSR, 55-57 bpm, no QTc prolongation 15:24: ventricular fibrillation 15:33: ventricular fibrillation • No torsades de pointes documented. CK-27
Subject 200214256DE: Spontaneous Report: Fatal Ventricular Arrhythmia (3) • 14:57: normal sinus rhythm, 55-57 bpm, no QTc prolongation CK-28
Subject 200214256DE: Spontaneous Report: Fatal Ventricular Arrhythmia (4) • 15:24: reported as ‘torsades de pointes’ • Considered ventricular fibrillation on expert read CK-29
Subject 200214256DE: Spontaneous Report: Fatal Ventricular Arrhythmia (5) • 15:33: ventricular fibrillation CK-30