Download
1 / 29
320 likes | 402 Views
Explore the structure and function of the adrenal glands, focusing on steroid hormone synthesis, adrenal cortex layers, and genetic defects impacting adrenal steroidogenesis. Learn about the actions of mineralocorticoids like aldosterone and glucocorticoids such as cortisol.

E N D
Endocrine PhysiologyThe Adrenal Gland1 Dr. Khalid AlrRegaiey
Adrenal (Suprarenal) Glands • Adrenal glands – paired, pyramid-shaped organs atop the kidneys • Weigh 6-10 g. • Structurally and functionally, they are two glands in one • Adrenal cortex (80-90%)– glandular tissue derived from embryonic mesoderm • Adrenal medulla (10-20%)– formed from neural ectoderm, can be considered a modified sympathetic ganglion
Adrenal Cortex • Synthesizes and releases steroid hormones (corticosteroids) • Different corticosteroids are produced in each of the three layers: • Zona glomerulosa – mineralocorticoids (mainly aldosterone) • Zona fasciculata – glucocorticoids +Androgens(mainly cortisol and corticosterone) • Zona reticularis – gonadocorticoids + glucocorticoids (mainly dehydroepiandrosterone DHEA)
Steroid Hormones Synthesis • Steroids are derivatives of cholesterol • Cholesterol is from the lipid droplets in cortical cells (cholesterol esters in LDL) • Removed cholesterol is replenished by cholesterol in LDL in blood or synthesized from acetate
Steroid Hormones Synthesis (Cont.) • Steroid hormones are synthesized and secreted on demand (not stored) • The first and rate-limiting step in the synthesis of all steroid hormones is conversion of cholesterol to pregnenolone by the enzyme cholesterol dismolase (aka cholesterol side chain cleavage (SCC) enzyme • Newly synthesized steroid hormones are rapidly secreted from the cell • Following secretion, all steroids bind to some extent to plasma proteins: CBG and albumin
Genetic Defects in Adrenal Steroidogenesis • Congenital adrenal hyperplasia cortisol ACTH ِAdrenal hyperplasia • 21-hydroxylase (P450c21) deficiency: cortisol, corticosterone, and aldosterone deficiency *ACTH Adrenal hypertrophy and high amounts of androgen * Virilization of female (masculanization)
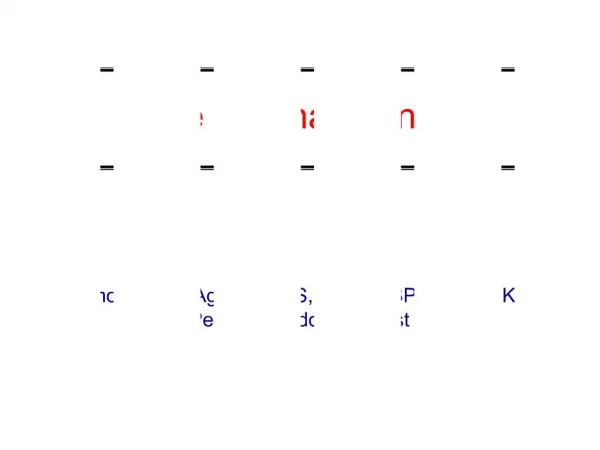
CH3 CH3 O O O C C OH HO HO HO CH3 CH3 O O O C C OH O O O CH2OH CH2OH O C O C OH O O CH2OH CH2OH O O C C OH HO HO O O Congenital Adrenal Hyperplasia: 21β- Hydroxylase Deficiency 17a-Hydroxylase (P450 c17) 17, 20 Lyase (P450 c17) Cholesterol ACTH Cholesterol desmolase (P450 scc) Pregnenolone 17-Hydroxypregnenolone Dehydroepiandrosterone 3b-Hydroxysteroid dehydrogenase 17-Hydroxyprogesterone Progesterone Androstenedione 21b-Hydroxylase (P450 c21) 11-Deoxycortisol 11-Deoxycorticosterone Testosterone 11b-Hydroxylase (P450 c11) Estradiol Cortisol Corticosterone
CH3 CH3 O O O C C OH HO HO HO CH3 CH3 O O O C C OH O O O CH2OH CH2OH O C O C OH O O CH2OH CH2OH O O C C OH HO HO O O Congenital Adrenal Hyperplasia: 11β- Hydroxylase Deficiency 17a-Hydroxylase (P450 c17) 17, 20 Lyase (P450 c17) Cholesterol ACTH Cholesterol desmolase (P450 scc) 17-Hydroxypregnenolone Pregnenolone Dehydroepiandrosterone 3b-Hydroxysteroid dehydrogenase 17-Hydroxyprogesterone Progesterone Androstenedione 21b-Hydroxylase (P450 c21) 11-Deoxycortisol 11-Deoxycorticosterone Testosterone 11b-Hydroxylase (P450 c11) Estradiol Cortisol Corticosterone
Mineralocorticoids • Synthesized in zona glomerulosa • Regulate the electrolyte concentrations of extracellular fluids • Aldosterone – most important mineralocorticoid • Maintains Na+ balance by reducing excretion of sodium from the body
Mineralocorticoids: Aldosterone • A steroid hormone. • Essential for life. • Responsible for regulating Na+ reabsorption in the distal tubule and the cortical collecting duct • Target cells are called “principal (P) cell”. • It also affects Na+ reabsorption by sweat, salivary and intestinal cells. * Stimulates synthesis of more Na/K-ATPase pumps.
Aldosterone exerts the 90% of the mineralocorticoid activity. Cortisol also have mineralocorticoid activity, but only 1/400th that of aldosterone. - Secreted by Zona glomerulosa. Aldosterone contin.
Corticosteroids & Their Relative Glucocorticoid & Mineralocorticoid Activities Compared to Cortisol Average Plasma Concentration (free and bound, μg/100 ml) Average Amount Secreted (mg/24 hr) Glucocorticoid Activity Mineralocorticoid Activity Steroids Adrenal Steroids Cortisol Corticosterone Aldosterone Deoxycorticosterone Dehydropiandrosterone Synthetic Steroids Cortisone Prednisolone Methylprednisone Dexamethasone 9α-fluorocortisol 12 0.4 0.006 0.006 175 __ __ __ __ __ 15 3 0.15 0.2 20 __ __ __ __ __ 1 0.3 0.3 0.2 __ 0.7 4 5 30 10 1 15.0 3000 100 __ 1.0 0.8 __ __ 125 Table 77-1, Guyton & Hall
Aldosterone Actions Maintains extracellular fluid volume by conserving body sodium. Aldosterone stimulates sodium & potassium transport in sweat glands, salivary glands, & intestinal epithelial cells.
Actions of Aldosterone Stimulates sodium reabsorption by distal tubule and collecting duct of the nephron and promotes potassium and hydrogen ion excretion • Increases transcription of Na/K pump • Increases the expression of apical Na channels and an Na/K/Cl cotransporter • By osmosis, water is also retained which expands ECF volume
Aldosterone Actions Aldosterone stimulates the active secretion of potassium from the tubular cell into the urine. Most potassium that is excreted daily results from distal tubular secretion. Hence aldosterone is critical for disposal of daily dietary potassium load at normal plasma potassium concentrations. Stimulates secretion of H+ by the kidney.
Regulation of Aldosterone Release 1. Increased potassium ion concentration in the extracellular fluid greatly increases aldosterone secretion. 2. Increased activity of the renin-angiotensin system (increased levels of angiotensin II) also greatly increases aldosterone secretion. 3. Increased sodium ion concentration in the extracellular fluid very slightly decreases aldosterone secretion. 4. ACTH from the anterior pituitary gland is necessary for aldosterone secretion but has little effect in controlling the rate of secretion.
Principal factor controlling Ang II levels is renin release. Decreased circulating volume stimulates renin release via: - Decreased BP (symp effects on JGA). Decreased [NaCl] at macula densa (“NaCl sensor”) - Decreased renal perfusion pressure (“renal” baroreceptor) Renin-angiotensin-aldosterone system
Lack of aldosterone: Increased sodium, chloride, water loss Decrease ECF volume Hyperkalemia Mild acidosis Plasma sodium decreases and may lead to circulatory collapse. Decrease cardiac output – shock - death within 4 days to a 2 weeks if not treated. Cardiac toxicity Hypoalsosteronism
Hyperaldosteronism can be caused by: Primary overproduction of aldosterone in conditions such as Conn’s syndrome. Conditions of low cardiac output are also known to stimulate synthesis of aldosterone. Both conditions result in sustained hypertension. Hyperaldosteronism
Hypertension. Hypokalemia Nocturnal polyuria & polydipsia Increased tubular (intercalated cells) hydrogen ion secretion, with resultant mild alkalosis. Neuromuscular manifestations weakness, paresthesia intermittent paralysis Clinical features of Hyperaldosteronism
Overproduction of aldosterone • treatment • surgical for adenoma • medical with Spironolactone