Download
1 / 66
680 likes | 1.06k Views
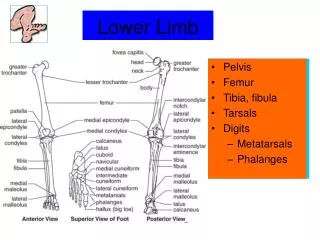
Clinical anatomy of the upper limb. Kaan Yücel M.D., Ph.D . 20.March.2012 Tuesday. CLINICAL ANATOMY OF THE AXILLA. Enlargement of Axillary Lymph Nodes. Lymphangitis ( inflammation of lymphatic vessels ) Cause : An infection in the upper limb

E N D
Clinical anatomy of the upper limb Kaan Yücel M.D., Ph.D. 20.March.2012 Tuesday
CLINICAL ANATOMY OF THE AXILLA
Enlargement of AxillaryLymphNodes Lymphangitis (inflammation of lymphaticvessels) Cause: An infection in the upperlimb Humeralgroup – firstto be involved
Enlargement of AxillaryLymphNodes Metastaticcancer of the apicalgroup adheretoaxillaryvein excisionof part of the axillaryvein • Enlargement of the apicalnodes • obstruction of the cephalicvein • superiortopectoralisminor
ArterialInnervationandRaynaud’sDisease • The arteries of the upperlimbareinnervatedbysympatheticnervesthrough the brachialplexus. • Vasospasticdiseasesinvolvingdigitalarterioles, suchas Raynaud’sdisease, mayrequire a cervicodorsalpreganglionicsympathectomytopreventnecrosis of the fingers. • The operation is followedbyarterialvasodilatation, withconsequentincreasedbloodflowto the upperlimb.
Aneurysm of AxillaryArtery The firstpart of the axillaryarterymayenlarge (aneurysm of the axillaryartery) andcompress the trunks of the brachialplexus, causingpainandanesthesia (loss of sensation) in the areas of the skin suppliedby the affectednerves.
SpontaneousThrombosis of the AxillaryVein Spontaneousthrombosis of the axillaryveinoccasionallyoccursafterexcessiveandunaccustomedmovements of the arm at the shoulderjoint.
CLINICAL ANATOMY OF THE BRACHIAL PLEXUS
DermatomesandCutaneousNerves of the UpperLimb Checking the integrity of the spinalcordsegments on the skin Dermatome: Skin areasuppliedby a spinalsegment C3-C6lateralmargin of the limb C7 middlefinger C8-T2 medialmargin of the limb
ShoulderPain • The skin over the point of the shoulderandhalfwaydown the lateralsurface of the deltoidmuscle is suppliedby the supraclavicularnerves (C3 and 4) • The afferentstimulireach the spinalcordvia the phrenicnerves (C3, 4, and 5). • Differentialdiagnosis time • Inflammatorylesionsinvolving the diaphragmaticpleuraorperitoneum • Pleurisy • Peritonitis • Subphrenicabscess • Gallbladderdisease
BrachialPlexusInjuries Complete lesionsinvolvingall the roots of the plexusarerare. Incompleteinjuriesarecommonandareusuallycausedbytractionorpressure; individualnerves can be dividedbystabwounds.
UpperLesions of the BrachialPlexus (Erb-DuchennePalsy) Excessivedisplacement of the headto the oppositeside & depression of the shoulder on the sameside. Result-Excessivetraction or even tearing of C5 and 6 roots Infantsduring a difficultdelivery Inadultsafter a blowtoorfall on the shoulder The actor Martin Sheen, however, is on record as mentioning a birth accident in which forceps "mangled" his shoulder. shoulderdystocia
Nervesderivedfrom C5 & C6 rootsaffected SuprascapularnerveNerveto the subclavius MusculocutaneousnerveAxillarynerve • Musclesparalyzed • Supraspinatus (abductor of the shoulder) • Infraspinatus(lateralrotator of the shoulder) • Subclavius(depresses the clavicle) • Bicepsbrachii(supinator of the forearm, flexor of the elbow, weakflexor of the shoulder) • Greaterpart of the brachialis(flexor of the elbow) • Coracobrachialis (flexor of the shoulder) • Deltoid(abductor of the shoulder) • Teres minor(lateralrotator of the shoulder)
Limbhangingbythe side Mediallyrotated [unopposedsternocostalpart of pectoralismajor] Forearmpronatedlossof bicepsbrachiiaction Waiter’stip position Lossof sensationdown the lateralside of the arm
LowerLesions of the BrachialPlexus (KlumpkePalsy) Usuallytractioninjuriescausedbyexcessiveabduction of the arm First thoracicnerve Median & ulnarnerves Hand- Clawedappearance Hyperextension of metacarpophalangealjoints Flexionof interphalangealjoints Lossof sensationmedialside of the arm C8 nervedamaged, medialside of the forearm, hand, andmedialtwofingers.
LongThoracicNerveInjuries Serratusanteriormuscle Blowstoorpressure on the posteriortriangle of the neck Duringthe surgicalprocedure of radicalmastectomy Difficultyin raising the armabove the head. Wingedscapula The vertebralborder& inferiorangle of the scapulawillnolonger be keptcloselyappliedto the chestwallandwillprotrudeposteriorly
AxillaryNerveInjuries Posteriorcord of the brachialplexus (C5 & 6) Pressureof a badlyadjustedcrutchpressingupwardinto the armpit Vulnerable @ quadrangularspace Downwarddisplacement of the humeralhead in shoulderdislocations Fracturesof the surgicalneck of the humerus
AxillaryNerveInjuries Deltoid & teres minorparalysis Lossof skin sensationover the lowerhalf of the deltoidmuscle
RadialNerveInjuries @Axilla • Badlyfittingcrutchpressingupinto the armpit • Drunkardfallingasleepwithonearmover the back of a chair • Fracturesanddislocations of the proximalend of the humerus • Motor • Triceps,anconeus, extensors of the wristparalyzyed • No extension of elbow, wrist & fingers • Wristdrop- flexion of the wrist • Supination ok intactbicepsbrachii (musculocutaneousnerve)
RadialNerveInjuries @ Axilla Sensory A smallloss of skin sensation Downposteriorsurface of lowerpart of the arm Downa narrowstrip on the back of the forearm Variablearea of sensorylosson the lateralpart of the dorsum of the hand&on the dorsalsurface of the roots of the lateral3 ½ fingers. Areaof total anesthesia relativelysmall becauseof the overlap of sensoryinnervationbyadjacentnerves
RadialNerveInjuries @ Spiral Groove of Humerus Fractureof the shaft of the humerus The pressure of the back of the arm on the edge of the operatingtable Mostcommon@ distalpart of the groove Motor Wristdrop Sensory Variablesmallarea of anesthesiaoverthe dorsalsurface of the hand& dorsalsurface of the roots of 3 ½ fingers
RadialTunnelSyndrome • Tenderness & pain the forearmjustbelow the elbow • Watch outfor • lateralepicondylitis(tenniselbow) • Differentialdiagnosismadeon history & physicalexam • The differencebetweenthesetwoconditions: where the elbow is most tender • Lateralto the elbow the radialnervetravelsbelow the supinatormuscle
TennisElbow (Lateralepicondiylitis) • Small area of chronicpain@ lateralelbow • Painon wristextension, painwhenshakinghands, weakened grip • Morecommon 30 -50 yrs of age • Manyconditionsfor the cause; • not onlytennis • Repeateduse of of the forearmextensormuscles • extensorcarpiradialisbrevis • lateralepicondyleto 2nd metacarpal
Injuries to the Deep Branch of the Radial Nerve Motor nerveto the extensormuscles in the posteriorcompartment of the forearm Fracturesof the proximalend of the radius Dislocationof the radialhead No sensoryloss- Motor nerve Supinator(posteriorinterosseusnervecontinuation of deepbranch) & extensorcarpiradialislongus (radialnerve)undamaged, andbecause the lattermuscle is powerful, it willkeep the wristjointextended, andwristdropwill not occur.
Injuries to the Superficial Radial Nerve Sensory As in a stabwound; A variablesmallarea of anesthesiaover the dorsum of the hand& dorsalsurface of the roots of the lateral3 ½ fingers
MusculocutaneousNerveInjuries • Rarelyinjured • Protectedbeneaththe bicepsbrachiimuscle • Injuredhighup in the arm; • Biceps & coracobrachialisparalyzedbrachialismuscle is weakened(alsosuppliedbyradialnerve). • Flexion of the forearm at the elbowproducedby the remainder of the brachialis& flexorsof the forearm.
MusculocutaneousNerveInjuries Sensorylossalong the lateralside of the forearm lateralcutaneousnerve of the forearm continuationof the musculocutaneousnervebeyond the cubitalfossa
MedianNerveInjuries Occasionallyin the elbowin supracondylarfractures of the humerus Mostcommonlyinjuredbystabwoundsorbrokenglass proximalto the flexorretinaculum: Here it lies in the intervalbetween the flexorcarpiradialis& flexordigitorumsuperficialistendons, overlappedby the palmarislongus.
MedianNerveInjuries @ the Elbow • Motor • Pronatormuscles of the forearm • Longflexormuscles of the wrist& fingers • paralyzed • Exception • flexorcarpiulnaris& medialhalf of flexordigitorumprofundus • Forearm in supineposition; weakwristflexionaccompaniedbyadduction • No flexion@ interphalangealjoints of the index& middlefingers
MedianNerveInjuries @ the Elbow Orator’shandposture • Ask the patienttomake a fist • Index finger, lesserextentmiddlefingerstraight • Ring & littlefingersflex • No flexion @ thumb’s terminal phalanx • flexorpollicislongusparalysis • Thenareminenceflattened • thenarmuscleswasted • Thumblaterallyrotated& adducted • Handflattened • «ape-like» hand
MedianNerveInjuries @ the Elbow Sensory Skin sensationloss Lateralhalforless of the palm of the hand Palmaraspect of lateral 3 ½ fingers VasomotorChanges Warmer & drier skin arteriolardilatationandabsence of sweatingresultingfromloss of sympatheticcontrol TrophicChanges Dry skin andscaly Nailscrackeasily Atrophy of the pulp of the fingers
MedianNerveInjuries @ the Wrist Motor Thenarmusclesparalyzed Thenareminenceflattened Thumblaterallyrotated & adducted No opposition of the thumb «ape-like» hand First twolumbricalsparalyzed When the patientis askedtomake a fistslowly, index & middlefingerstendtolagbehind the ring & littlefingers.
MedianNerveInjuries Perhapsmostseriousdisabilityof all in mediannerveinjuries: Lossof abilitytooppose the thumbtothe otherfingers Lossof sensationover the lateralfingers Delicatepincer-likeaction of the hand is nolongerpossible.
UlnarNerveInjuries Mostcommonlyinjured at the elbow where it liesbehind the medialepicondyle usuallyassociatedwithfractures of the medialepicondyle Mostcommonlyinjured at the wrist whereit lieswithulnararteryin front of flexorretinaculum
UlnarNerveInjuries @ the Elbow • Motor • Flexorcarpiulnaris& medialhalf of the flexordigitorumprofundusparalyzed • ASK YOUR PATIENT TO MAKE A FIST • No observation/thightening of the flexorcarpiulnaristendonpassingto the pisiform bone • No fxn of theprofundustendons • No flexion of ring & littlefingers’ terminal phalanges • Flexionof the wristjointwillresult in abduction, owingtoparalysis of the flexorcarpiulnaris.
UlnarNerveInjuries @ the Elbow Medialborder of the front of the forearmflattens wastingof underlyingulnaris& profundusmuscles Small muscles of the handparalyzed exceptthenarmuscles & first 2 lumbricals -mediannerve-
UlnarNerveInjuries @ the Elbow Unableto grip a piece of paperplacedbetweenthefingers No adduction & abduction of fingers No adductthethumb Paralyzedadductorpollicis Extensordigitorumabductfingersto a smallextent, whenmetacarpophalangealjointshyperextended FROMENT’S SIGN Ask yourpatienttogrip a piece of paperbetweenthethumb& indexfinger: S/he doessobystronglycontractingflexorpollicislongus& flexingthe terminal phalanx
UlnarNerveInjuries @ the Elbow • Metacarpophalangealjointshyperextended • Interphalangealjoints • flexed • Lumbrical & interosseousmusclesparalysis • 4th & 5th fingers
UlnarNerveInjuries @ the Elbow • Inlongstandingcases the handassumes the characteristic “claw” deformity(Main en griffe). • Flatteningof the hypothenareminence • Lossof the convexcurveto the medialborder of thehand • Examinationof the dorsum of thehand: • Hollowingbetween the metacarpalbonescausedbywasting of the dorsalinterosseousmuscles.
UlnarNerveInjuries @ the Elbow • Sensory • Loss of skin sensation • Anterior & posteriorsurfaces of the medialthird of thehand • Medial 1 ½ fingers • VasomotorChanges • Warmeranddrierskin • arteriolardilatation& absence of sweating • resultingfromloss of sympatheticcontrol
UlnarNerveInjuries @ the Wrist Motor Small muscles of thehand-exceptthenar & first 2 lumbricals Clawhandmoreobvious flexordigitorumprofundusnot paralyzed, markedflexion of terminal phalanges
UlnarNerveInjuries @ the Wrist • Sensory • Main ulnarnerve& itspalmarcutaneousbranchusuallysevered • Posteriorcutaneousbranch, arisesfrom the ulnarnervetrunkabout 2.5 in. (6.25 cm) above the pisiformbone usuallyunaffected • Sensorylossconfinedto • Palmarsurface of medial1/3 of the hand • Medial 1 ½ fingers • Dorsalaspects of middle& distalphalangesof thesamefingers
UlnarNerveInjuries • Withulnarnerveinjuries, • thehigher the lesion is the lessobvious is the clawingdeformity of the hand. • Unlikemediannerveinjuries, lesions of the ulnarnerveleave a relativelyefficienthand. • Sensationover the lateralpart of the hand is intact, pincer-likeaction of the thumbandindexfinger is reasonablygood, althoughthere is someweakness, owingtoloss of the adductorpollicis.
CLINICAL ANATOMY OF THE SHOULDER
Quadrangular Space Syndrome • Compression of axillarynerve& posteriorcircumflexhumeralartery@ quadrilateralspace • Downwarddisplacement of the humeralhead in shoulderdislocations • Fracturesof the surgicalneck of the humerus • Deltoid & teres minorparalysis • Lossof skin sensationlowerhalf of deltoidmuscle
RotatorCuffTendinitis Stabilizing the shoulderjoint Commoncause of pain in the shoulder Excessiveoverheadactivity of the upperlimbmay be the cause of tendinitis, althoughmanycasesappearspontaneously.
RotatorCuffTendinitis Subacromial bursa-Supraspinatus Goodfor the ease of frictionduringabduction of the shoulder Subacromialbursitis, supraspinatustendinitis, orpericapsulitis Characterizedby the presence of a spasm of pain in the middlerange of abduction, when the diseasedareaimpinges on the acromion.
Rupture of the SupraspinatusTendon • Inadvancedcases of rotatorcufftendinitis, the necroticsupraspinatustendon can becomecalcifiedorrupture. • Inabilitytoinitiateabduction of the arm • However, if the arm is passivelyassistedfor the first 15° of abduction, the deltoid can thentakeoverandcomplete the movementto a rightangle.