Download
1 / 47
490 likes | 696 Views
Meaningful Use of Electronic Health Records. Sarah Chouinard, MD. Community Care of WV, CMO WVRHITEC, Medical Director. Objectives for the Webinar. Define Meaningful Use and be able to identify the main regulatory objectives of MU

E N D
Meaningful Use of Electronic Health Records Sarah Chouinard, MD. Community Care of WV, CMO WVRHITEC, Medical Director
Objectives for the Webinar • Define Meaningful Use and be able to identify the main regulatory objectives of MU • Discuss why it is important to us as the future of medicine evolves • Discuss the transformational changes are necessary at the practice level to make meaningful use work
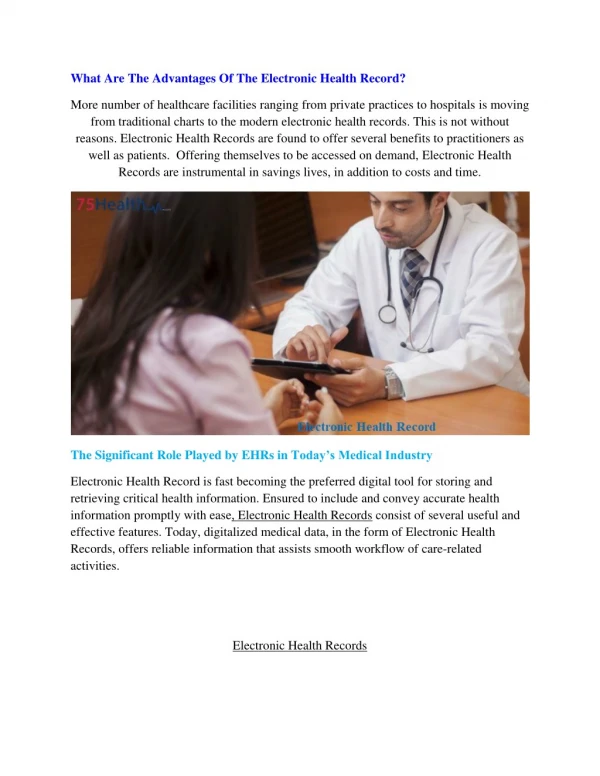
Definition of Meaningful Use • Use of certified electronic medical records to accomplish specific goals • Meaningful Use was defined by CMS in response to the Health InformationTechnology for Economic and Clinical Health Act (HITECH) • While there are legal and financial issues closely tied to meaningful use, the key goal is to digitize the practice of medicine in a way that is meaningful. Meaningful means patients have better health outcomes and more efficient, less redundant, safer care.
Why are we doing this? Money or something else? • Yes there are incentives, but the reason the incentive plan was created was to get providers to adopt technology and use it to improve care by meeting certain goals. • For those groups who meet these goals incentive payments will be awarded. By 2015 those who have not implemented meaningful use will NOT receive 100% of the fee schedule for their professional services from Medicare.
This is NOT about the money, but why not take it if $ is on the table? • 2011-2016 (Medicare) – up to $44,000 per provider over 5 years per provider for complete adoption of meaningful use • 2011-2021 (Medicaid)- up to $63,750 per provider over 6 years • 2015 and later- if not meaningful EMR user up to 3% payment adjustment in Medicare reimbursement
The 3 Stages of Meaningful Use • Stage1: (2011) Data capture, basic clinical functions, measure reporting • Stage 2: (2013) expands Stage 1, disease management measures • Stage3: (2015) Health Information exchange, population management, Clinical Decision Support
The Guidelines • The Final Rule was released on 7/13/10 • The Final Rule only refers to 2011-2012 • The meaningful use objectives have two parts: • The Core Set—required objectives • The Menu Set--providers will pick measures of interest to implement in the first two years
Objectives and Measures • There are 15 Core Objectives • Within each Objective there are Measures that can be counted and are used to assess whether meaningful use is being achieved
15 Core Objectives and Their Measures • Objective 1: Record patient demographics: age, sex, ethnicity, DOB, preferred language • Measure: More than 50% of patients have their demographics entered as structured data in EMR
Objectives • Objective 2: Record vital signs and chart changes (height, weight, blood pressure, body mass index, growth charts for children) • Measure: more than 50% of patients over 2 yrs of age have height, weight and blood pressure recorded as structured data
Objectives • Objective 3: Maintain an up-to-date problem list of current and active diagnoses • Measure: more than 80% of patients have at least one entry recorded as structured data
Objectives • Objective 4: Maintain an active medication list • Measure: more than 80% of patients have at least one entry recorded as structured data (no medications would count if recorded)
Objectives • Objective 5: Maintain an active medication allergy list • Measures: more than 80% of patients have at least one entry recorded as structured data
Objectives • Objective 6: Record smoking status for patients 13 years and older • More than 50% of patients 13 years and older have smoking status recorded as structured data
Objectives • Objective 7: Provide patients with a clinical summary for each office visit • Measure: clinical summaries provided to at least 50% of patients within 3 business days
Objectives • Objective 8: On request, provide patients with an electronic copy of their health information (including diagnostic test results, problem list, medication list, medication allergy list) • Measure: provide more than 50% of patients with their health information within 3 business days of the request
Objectives • Objective 9: Generate and transmit permissible prescriptions electronically • Measure: More than 40% of permissible prescriptions are transmitted electronically
Objectives • Objective 10: Computer Provider Order Entry (CPOE) for medication orders • Measure: At least 30% of patients with at least one medication in their medication list has been ordered through CPOE
Objectives • Objective 11: Implement Drug-Drug and Drug-Allergy checks • Measure: Functionality for these checks is enabled for the entire reporting period
Objectives • Objective 12: Implement capability to electronically exchange key clinical information among providers and patient-authorized entities • Measure: Perform at least one test of the EHRs capability to electronically exchange information
Objectives • Objective 13: Implement one clinical decision support rule and ability to track compliance with the rule • Measure: One clinical decision support rule implemented
Objectives • Objective 14: Implement systems to protect privacy and security of patient data in the EHR • Measure: conduct or review a security risk analysis, implement security updates as necessary, and correct identified security deficiencies
Objectives • Objective 15: Report clinical quality measures to CMS or States • For 2011 provide aggregate numerator and denominator through attestation, for 2012 report electronically
Menu Items • 10 total Items • Providers pick 5 of these items to implement between 2011-2012 for meaningful use • Eventually all 10 will be adopted
Menu Items • Menu #1 Objective: Implement drug formulary checks • Measure: Drug formulary check is implemented and has access to at least one internal or external drug formulary during the entire reporting period
Menu Items • Menu #2 Objective: Implement clinical laboratory test results into EHR as structured data (i.e. NOT scanned) • Measure: more than 40% of clinical laboratory test are incorporated into EHR as structured data
Menu Items • Menu #3 Objective: Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach • Measure: Generate at least one listing of patients with a specific condition
Menu Items • Menu #4 Objective: Use EHR technology to identify patient-specific educational resources and provide those to the patient as appropriate • Measure: more than 10% of patients are provided patient-specific educational resources
Menu Items • Menu #5 Objective: Perform medication reconciliation between care settings • Measure: medication reconciliation is performed in more than 50% of transitions of care
Menu Items • Objective #6 Objective: Provide summary of care record for patients referred or transitioned to another provider or setting • Measure: Summary of care provided for at least 50% of transitions or referrals
Menu Items • Menu #7 Objective: submit electronic immunization data to immunization registries or immunization information systems • Measure: Perform at least one test of data submission and follow-up submission (where registries can accept electronic submission)
Menu Items • Menu #8 Objective: Submit electronic syndromic surveillance data to public health agencies • Measure: Perform at least one test of data submission and follow-up submission (where public health agencies can accept electronic submission)
Menu Items • Menu #9 Objectives: Send reminders to patients (per patient preference) for preventative and follow-up care • Measure: More than 50% of patients 65 years or older or 5 years and younger are sent appropriate reminders
Menu Items • Menu #10 Objective: Provide patients with timely electronic access to their health information (including laboratory results, problem list, medications, medication allergies) • Measure: More than 10% of patients are provided electronic access to information within 4 days of it being updated in the EHR
Additional Guidelines • In 2011-2012 providers are also required to report 3 core quality measures: • Blood pressure level • Tobacco status • Adult weight screening and follow-up • (or alternates if these do not apply e.g. pediatrician)
How we will accomplish this task? • 1. A certified electronic health record is a must. Meaningful Use cannot be achieved on paper. • 2. How do we know if an EHR is certified? The WVRHITEC will provide us with guidance on certified vendors. • 3. Once we select an EHR, how do we know how to get the information in so that we can later get it out?
Quality Improvement = Input, Output, Outcomes, Out-smart • Input = Key clinical data must be put into a place where it can be pulled out of the EHR. If a provider documents a diabetic foot exam in an office note, the EHR might not be able to pull that exam out of the note. The exam might need to be documented in a place in the system where data can be stored for future reporting. Know thy system. Know thy EHR. Have a plan. • Output = How do you get info out once you put it in? • Outcomes = How will you know how many of your diabetics have (not) had a foot exam? • Out-smart = Is there a better way than flow sheets and chart auditing?
What is Continuous Quality Improvement (CQI)? • Many of us feel like we are continuously trying to improve, but CQI is much more than trying to be our best with the patients we see on a daily basis. • If everyone gets on board with trying to meet the goals of meaningful use, we will have a system where technology is used to manage patients in the context of the communities in which they live. By viewing patients in populations, we can watch trends in their wellness and chronic disease management. These observed trends are only possible with computers used to collect data, and report it back to the care providers. The health outcomes observed (the data) can be improved upon by continually trying to improve heath outcomes through outreach and patient engagement.
Demonstrating improvement in outcomes is the cornerstone of Meaningful Use. • Practitioners, who consistently assure that the process of care is intact, should expect certain outcomes from that care delivery. An electronic system should capture and report on the outcomes of that effort – not only for each patient, but for the population the practitioner serves • These outputs are then used to develop improvements in the delivery of care so that the process of care is supported, improve the individual practitioners approach and practice of medicine, and improve the patient satisfaction with the care they receive.
What does self management really mean? • Patients spend very little time in front of their health care providers every year. If a diabetic sees their doctor for a visit every 3 months for 20 minutes, that means the doctor patient “relationship” consists of less than 1.5 hours annually. • Patients need to know how to manage their health the other 361 days a year. • Remember “Out-smart”-ing the current way we practice? Well…
Providers cannot do this alone. We need to engage our patients. • Education—built in guideline in the EHR • Reminders—help care teams max pack visits • Outreach—contacting patients to remind them about services due • Personal Health Records—allow patients convenient access to their chart • e-Rx • Self-monitoring—proving tools for monitoring such as action plans • Clinical Summaries—give patients written information so that they have a clear knowledge of what was determined at the close of an office visit.
Closing Thoughts • Most guidelines asked for in Meaningful Use are clinically reasonable and will improve patient care. • Some guidelines are just a matter of using an EHR • Some guidelines, like lab values, require interfaces which can be technically challenging and require specialized expertise
Closing Thoughts Continued: • Practitioners, who consistently assure that the process of care is intact, should expect certain outcomes from that care delivery. An electronic system should capture and report on the outcomes of that effort – not only for each patient, but for the population the practitioner serves • These outputs are then used to develop improvements in the delivery of care so that the process of care is supported, improve the individual practitioners approach and practice of medicine, and improve the patient satisfaction with the care they receive. • Demonstrating improvement in outcomes is the cornerstone of Meaningful Use and actually, all clinical practice.
The time is now! • There is no question that implementing an EHR is expensive and time consuming. Implementing the new process of care required to achieve meaningful use is even more labor intensive than EHR implementation. • However, there has never been a better time to do it. Costs can now be offset by the HITECH payments and specific guidelines are now set so that we move forward together in the medical community.
Next Webinar November 17“Workflow and Staff Role Changes To Consider With An EHR” SystemTime: 12 noon to 1 p.m.Presenter: Dr. Sarah Chouinard, Primary Care Systems and W.Va. Regional HIT Extension Center Webinars Being Planned: MU BMS and CMS registration and attestation processes EHR Vendors and Offerings Privacy and security
The West Virginia Regional Health Information Technology Extension Center (WVRHITEC) was created as part of a national program by the Office of National Coordinator for Health Information Technology/U.S. DHHS. It has been established as part of the federal stimulus plan and is operating under the West Virginia Health Improvement Institute (http://www.wvhealthimprovement.org . This project is supported by Grant Number 90RC0017/01 from the Office of the National Coordinator, Department of Health and Human Services.
Questions? info@wvrhitec.org