Download
1 / 54
570 likes | 1.07k Views
Rotator Cuff Disease. Current Surgical Management. Chris Pullen. Historical Aspects. Codman in 1934 Impingement syndrome Arthroscopic SAD. Shoulder Arthroscopy. Rotator Cuff Disease. Tendinopathy/Impingement Rotator Cuff Tear Cuff Tear Arthropathy.

E N D
Rotator Cuff Disease Current Surgical Management Chris Pullen
Historical Aspects • Codman in 1934 • Impingement syndrome • Arthroscopic SAD
Rotator Cuff Disease Tendinopathy/Impingement Rotator Cuff Tear Cuff Tear Arthropathy
PTT –Surgery • Open • Mini – open • Arthroscopic*
PTT - Arthroscopy • Advantages • Visualisation • Treatment • articular tears
PTT - Arthroscopy • Bursal surface tear • SAD • Articular surface tear • Debridement only • Repair • >50% Thickness tear • Active patients
PTT - Arthroscopy • Results • Debridement +/- SAD • Repair
FTT - Surgical Approaches • Arthroscopic* • Arthroscopic assisted/mini-open* • Open
FTT - Arthroscopic RCR • Gleno-humeral Joint • PTT • Labral tears • Ligament injuries • Cartilage tears • Significant lesions in 12.5%
FTT – Arthroscopic RCR • Repair Site Preparation • Removal of ragged or degenerate tissue • Decortication of bone
FTT – Arthroscopic RCR • Suture Placement
FTT – Arthroscopic RCR • Anchor Placement • Foot print • Double row technique
FTT – Arthroscopic RCR • Other Tendon Lesions • Infraspinatus • Teres minor • Subscapularis • Biceps
FTT – Arthroscopic RCR • Biceps • Debridement • Tenotomy • Tenodesis
FTT – Arthroscopic RCR • Post – operative Treatment • Sling • Cryotherapy • PROM • AROM • Strengthening
FTT – Arthroscopic RCR • Results • 90% satisfaction • 78% pain relief • AROM
Massive Tears – Surgery • Debridement • Open • Arthroscopic* • Rotator Cuff Repair* • Tendon transfer* • Synthetic interposition • Arthrodesis • Arthroplasty
Massive Tears - Debridement • Debridement alone • Low demand patients • Results tend to deteriorate over time • Arthroscopic debridement • easier • more rapid rehabilitation
Massive Tears - Debridement • Limited acromioplasty • coracoacromial arch is maintained • Biceps tenotomy / tenodesis • subluxation, dislocation, or partial tearing • enhance the ability to alleviate shoulder pain
Massive Tears - RCR • Good function & pain relief 80-90% • Goal of surgery is to repair the cuff without disrupting the coraco-acromial arch
Massive Tears - RCR • Rehabilitation • Sling / Abduction splint • PROM • AAROM • Strengthening • Overall recovery may take >12 months
Massive Tears - RCR • Results • Inferior • Better within 6 weeks (Bassett & Cofield 1983) • Shoulder dislocation >40 • 85-90% good to excellent ( Bigliani 1992)
Massive Tears – Tendon transfer Latissimus Dorsi* Pectoralis Major* Teres Minor Subscapularis Deltoid muscle flap Trapezius
Massive Tears – Latissimus Dorsi • Supraspinatus/Infraspinatus loss • Restore ER & head depression forces
Massive Tears – Latissimus Dorsi • Results • 82% satisfactory (Miniaci & MacLeod 1999) • Intact subscapularis • Little or no restoration of strength in overhead activity
Massive Tears – Pectoralis Major • Subscapularis tears
Massive Tears - Reconstruction • Tissue implants • Autologous • Autogenous • Freeze-dried cadaveric tissue
CTA - Surgery Arthroscopic debridement* Humeral tuberoplasty Shoulder arthrodesis Total Shoulder Replacement Hemiarthroplasty* Reverse Shoulder Arthroplasty*
CTA - Hemiarthroplasty • Indications • <70 years • Active elevation >90° • CTA Head • Variation of the hemiarthroplasty
CTA - Hemiarthroplasty • Results • Functional results limited, pain relief is excellent (Williams & Rockwood 1996) • Zuckerman et al (2000) decreased pain, increased FF86 & ER 30. • Sanchez-Sotelo et al (2001) 67% successful at 5 year follow-up
CTA - Hemiarthroplasty • Results • intact coracoacromial arch essential
CTA- Reverse Shoulder Arthroplasty • Semiconstrained reverse ball and socket • Grammont 1985
CTA - RSA • Biomechanics (Boileau et al 2005) • Large glenosphere • Medialisation of the centre of rotation • Lowers humeral head
CTA - RSA • Indications • > 70 years or no active elevation • Low demand
CTA - RSA • Results (Boileau et al 2005, De Buttet et al 1997, Rittmeister et al 2001) • Excellent pain reduction • Improved active abduction
CTA - RSA • Complications • High • Rate revision is high (4.2-13%) • Not for the occasional operator
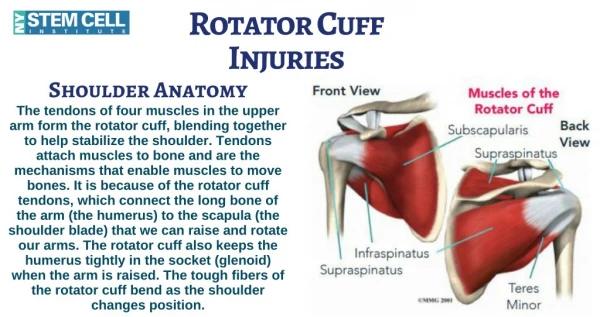
Rehabilitation -Biomechanics • Rotator Cuff • Stabilises gleno-humeral joint • Depresses the humeral head • Protective overlap • Subscapularis • Scapulo-thoracic dyskinesia • Compensatory impairment leads to winging • Alter orientation of the acromial arch
Rehabilitation – Tendon Healing • Spontaneous healing ?? • Phases • Inflammatory • Proliferative • Maturation • Maximal load to failure 12-26 weeks
Rehabilitation - Immobilisation Early ROM Abduction splint Shoulder immobilisation with an abduction-type splint for 4-6 weeks
Rehabilitation - Cryotherapy • Speer et al 1996 • Less pain 1st 24 post-operative hours • Better sleep • Lesser analgesic requirement • Less swelling • Better able to tolerate rehabilitation
Rehabilitation - PTT • Goals • Full ROM • Reducing impingement • Physical therapy plus exercise program better than exercise alone
Rehabilitation - RCR • Goals • Mobilise the joint early • Load the repaired tendons safely • Strengthen the rotator cuff progressively
Rehabilitation - RCR • Phases • Immediate post-operative period (week 0-6) • Protection & active ROM (week 6-12) • Early strengthening (week 10-16) • Advanced strengthening (week 16-22)
Rehabilitation – Phase 1 • Goals • Maintain / Protect repair integrity • Gradual increase PROM • Diminish pain & inflamation • Prevent muscle inhibition • Exercises • Sling/abduction splint 6 weeks • Immediate PROM (depends on repair tension) • Pendular exercises • Cryotherapy • Hydrotherapy