Download
1 / 44
440 likes | 666 Views
Fitness To Drive. Nellemarie Hyde, OT Reg. (Ont.); CDRS Beth Crystal, OT Reg. (Ont.). The Participants. Who has previously referred a client for a driving assessment? What types of diagnoses do your clients have? (stroke? ABI? amputation? SCI? MS? dementia?)

E N D
Fitness To Drive Nellemarie Hyde, OT Reg. (Ont.); CDRS Beth Crystal, OT Reg. (Ont.)
The Participants • Who has previously referred a client for a driving assessment? • What types of diagnoses do your clients have? (stroke? ABI? amputation? SCI? MS? dementia?) • Has anyone in whole or in part, conducted a driving assessment? • Prescreening for a driving assessment?
Objectives • Determining who is at risk for medically impaired driving • Mandatory reporting and MTO process • Comprehensive Driving Assessment: What to expect • Case Studies
Road back to Driving • Who is at risk for medically impaired driving?
Who is at risk? It is not age alone!! • It is medical conditions • Medical conditions and medications are the primary cause of declines in driver competence. • Can make even the best of drivers unsafe to drive. • Can affect drivers of any age: Increasingly likely as we age. • Medical community best positioned to first recognize possibly impairing medical conditions.
Medical Conditions Any medical condition that results in a change of physical, sensory, mental or emotional abilities has the potential to compromise driving performance. • Physical (weakness; limited movement etc) • Sensory (vision loss; limited feeling in limbs etc) • Cognitive/Perceptual (slowed thinking; attention etc) • Emotional (anxiety etc)
Increased Risk of an At-Fault Crash 7.6 5.0 5.0 Risk of an At-Fault Crash 2.8 3.0 2.5 2.1 2.2 1.8 Visual Acuity Pulmonary Psychiatric Diabetes Epilepsy BAC .08 Cardiovascular Cognitive Neurological
0% 10% 20% 30% 40% 50% 60% 70% 65-74 75-84 85+ Alzheimer’s Disease and Other Dementia Cognitive Impairment that is not Dementia Prevalence of Cognitive Impairment* AGE *(CSHA, 1991)
Highway Traffic Act 1990c. H. 8 Doctor reports to the MTO Section 203, (1) Mandatory Reporting for: “Every person 16 yrs. of age or over, attending upon the medical practitioner for medical services who, in the opinion of the medical practitioner, is suffering from a condition that may make it dangerous for the person to operate a motor vehicle.”
The Doctor’s Dilemma • Doctors are asked to report if a patient’s medical condition may affect their ability to drive • If this was carried out to the word, the MTO would likely be inundated with reports from doctors • Instead, doctors are left to determine, from their office, who should be reported to the MTO • OT’s offer valuable input to doctors
When MTO is Informed • The license may not be suspended. • A file is opened with the Medical Review Section. • The case is reviewed by an analyst. • MTO will determine the next course of action. • Once report is made it can take 4-6 weeks for response.
MTO course of action • may request medical information • go through the standard licensing procedure • may request a driving assessment from an approved rehabilitation facility • may suspend license on a medical basis (temporary licenses can be obtained for assessment and/or training)
Who should be assessed? • Collisions and/or damage to the car • Getting lost • Near-misses with vehicles, pedestrians • Confusing the gas and brake • Traffic tickets • Missing stop signs/lights; stopping for green light • Deferring right of way • Not observing when making lane changes, merging • Others honking/irritated with the driver • Needing a co-pilot
Who should be assessed? Physical Impairment: • Difficulty moving their body through the motions of driving (poor coordination, strength, range of motion) • Impaired reaction time
Who should be assessed? Cognitive/Perceptual Impairment • Impaired processing speed (>150 seconds on Trails B – may indicate increased crash risk) • Impaired visual perception (<30/40 on MVPT-R) • A history of left inattention or neglect • Impaired judgement, problem solving • Difficulty with IADLs or ADLs
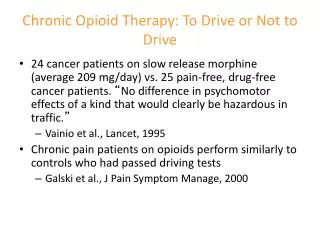
Who should be assessed? Psychological / Emotional Impairment • Driving anxiety • Psychomotor slowing • Cognitive deficits • Side effects from medications • Impaired judgement
Who should be assessed? Vision Deficits • Visual Acuity: minimum 20/50 with both eyes open • Visual Field: 120° continuous vision with 15° above and 15° below the visual field (60° to right and left) • MTO Vision Waiver Program for class G license for visual field impairment
Specialized Assessment The role of a Rehabilitation Driving Assessment: • Determine the impact of a medical condition on driving. • Recommend training and adaptive equipment if appropriate. • Support driving independence. • Monitor performance over time.
Specialized Assessment • In Ontario, an Occupational Therapist is required to conduct the assessment in order to be a Ministry Approved Facility. • The cost of assessment is not covered by the health care or licensing system – the client covers the cost. • Fees are approximately $500 - $600.
Driving Assessment In the Clinic (1.5-2 hours with OT): • Medical and Driving History • Vision Screen • Cognitive/Perceptual Assessment • Physical Assessment
Driving Assessment Cognitive/Perceptual Assessments • Cognistat or MMSE (as a screen) • MVPT-R or MVPT-3 • Useful Field of View (UFOV) • Trail Making A & B Or • DriveABLE Assessment
Driving Assessment In the Vehicle (Driver Rehab): • Given in dual-brake vehicle • Occupational Therapist and Certified Driving Instructor • In-clinic determines course of on-road assessment • Will abort drive if major errors arise
DriveABLE™ • DriveABLE™ -- developed through research. • Research won national award of excellence. • Alberta Heritage Foundation for Medical Research encouraged championing move from research to practice through the establishment of a University spin-off company -- DriveABLE™.
DriveABLE™ Cognitive/Perceptual Assessment • Completed on a computer • Touch Screen and push button response • Assesses areas of: • motor control - attention shifting • judgment - attentional field • executive function • On-road Assessment
DriveABLE™ In the Vehicle: • Given in dual-brake vehicle • Score only the competence defining errors • Road Course design reliably reveals the competence defining errors • Bad habit errors not scored • Protects the competent driver • Fail criterion is “Out of the range of normal”
Driving Assessment Recommendations are given and may include: • Continue Driving • Future Reassessment • Training • Discontinue Driving
Functional Vision Assessment • Began May 2005 • Only five MTO approved centres in Ontario (pilot) • Goal: to determine if the client can compensate for vision loss
Functional Vision Assessment If approved by MTO: • 2 hour clinical assessment (OT) • UFOV, CTMT, MVPT-3, Scan Course, Insight, physical assessment 1.5 hour on road assessment (OT and DI) • Two road tests: residential, main road, freeway, break in between to review
Functional Vision Assessment • Expectation on road is quite high • Blind spot checks on turns and lane changes • Anticipatory scanning • Speed of maneuvers • Use of mirrors • Client cannot miss more than two in any category on any particular maneuver
Functional Vision Assessment Recommendations include: • Able to compensate, recommend driving • Able to compensate, training in community • Did not compensate, training with MTO approved rehab facility • Unable to compensate due to inability and/or lack of insight, driving cessation recommended
Determining Medical Fitness to Operate Motor Vehicles • Published by the Canadian Medical Association • Addresses: • Functional Driving Assessment • Medical Reporting • Driving Cessation • Alcohol, Drugs • Aging • Sleep Disorders • Psychiatric Illness
Determining Medical Fitness to Operate Motor Vehicles • Addresses (continued): • Nervous System Impairments • Vision Deficits • Auditory-Vestibular Disorders • TBI and stroke • Vascular, cardiovascular and cerebrovascular diseases • Respiratory diseases, endocrine and metabolic disorders • Sections on general debility, anesthesia, surgery, seat belts and air bags
Determining Medical Fitness to Operate Motor Vehicles • Alert box • Overview • Detailed breakdown within each Section • Identifies where a functional driving assessment should be considered
Who should be assessed? • Case Studies
Case Study Amputation • 65 year old man with 16 year history of diabetes • Developed PVD in the (R) lower extremity 2 years ago • Right below knee amputation 3 months ago
Amputation • What are this gentleman’s options for driving? • What are the potential concerns regarding his driving options? • At what point in his rehab should he be referred for a driving assessment? • Who should inform the MTO and when?
Case Study Vision Deficit / CVA • 56 year old female sustained an occipital CVA one year ago • Visual field testing indicates a (L) homonymous hemianopia • Doctor notified MTO and her License was suspended while she was in the hospital • Client has asked if / when she will be able to resume driving
Vision Deficit • Can someone with HH be considered for driving? • What information/documentation will the MTO require? • Who can conduct this type of assessment? • What does the driving assessment entail?
Case Study Traumatic Brain Injury • 18 year old male sustained a severe TBI as a passenger in a MVA • At the time of the injury, he held a G1 license • Recent neuropsych testing shows deficits in attention, concentration, judgement • Family reports changes in his behaviour • He has expressed a desire to resume driving with his dad.
Traumatic Brain Injury • What red flags might the OT look for when considering the assessment? • Does he require a driving assessment or can he simply proceed through MTO testing? • At what point in his rehab should driving be considered? • Is it okay for him to practice driving with his dad?
Case Study Spinal Cord Injury • 38 year old male sustained a C5/6 spinal cord injury during an ATV roll over 6 months ago • Reports dizziness upon rising in the morning • Has expressed frustration with having to rely on Wheel Trans • Wishes to pursue driving
Spinal Cord Injury • Is this an appropriate referral? • At what point in his rehab should he be referred for a driving assessment? • What types of assessments might be appropriate at this time? • When should the MTO be advised of the medical condition?
Resources • Determining Medical Fitness to Operate Motor Vehicles; Canadian Medical Association Driver’s Guide 7th edition. (available online) • www.saintelizabeth.com (select “services”; “driver”) • www.driveable.com (for cognitive impairment) • Medical Review Section 416-235-1773 (client inquiries; for a list of assessment centres)
Thank you! Nellemarie Hyde, OT Reg. (Ont.); CDRS