Download

1 / 44
440 likes | 602 Views
Acute Pain Management in Times of Epidemic Prescription Drug Abuse. Rumm Morag, MD, FACEP Department of Emergency Medicine Salem Hospital. Objectives. U nderstanding the direct correlation between opiate sales and the prescription overdose death rate

E N D
Acute Pain Management in Times of Epidemic Prescription Drug Abuse Rumm Morag, MD, FACEP Department of Emergency Medicine Salem Hospital
Objectives • Understanding the direct correlation between opiate sales and the prescription overdose death rate • Utilize adjuvant non-opiate treatments for management of acute pain • To understand the role of the Oregon Prescription Drug Monitoring Program • Inform regarding IRON ED
What is Pain? • Pain is a real condition • An unpleasant sensory experience
Pain is… • Something different to every person • Does not show up on lab testing or imaging and may have no objective findings • So we must begin this discussion with definitions we can all agree upon…..
Defining Pain • Pain is subjective • Has physical and emotional components • Difficult to quantify • Common • Costly • Difficult to manage
Pain is common • The most common reason for physician consultation in the United States • The most common symptom presenting the Emergency Department • 42% of all Emergency Department visits are due to subjective pain Platter et al. JAMA. 2008;299:70-78
Pain is Political • Joint Commission calls pain the “fifth vital sign” • Emphasis on patient satisfaction (not outcomes) • IOM Report stresses “poor pain control by MDs” • Pain aversive culture expects “No Pain at all” • Public expectation to receive “Stronger Medication” Phillips DM, JCAHO standards. JAMA. 2000;284:428-429 IOM 2011, Washington DC: The National Academies Press
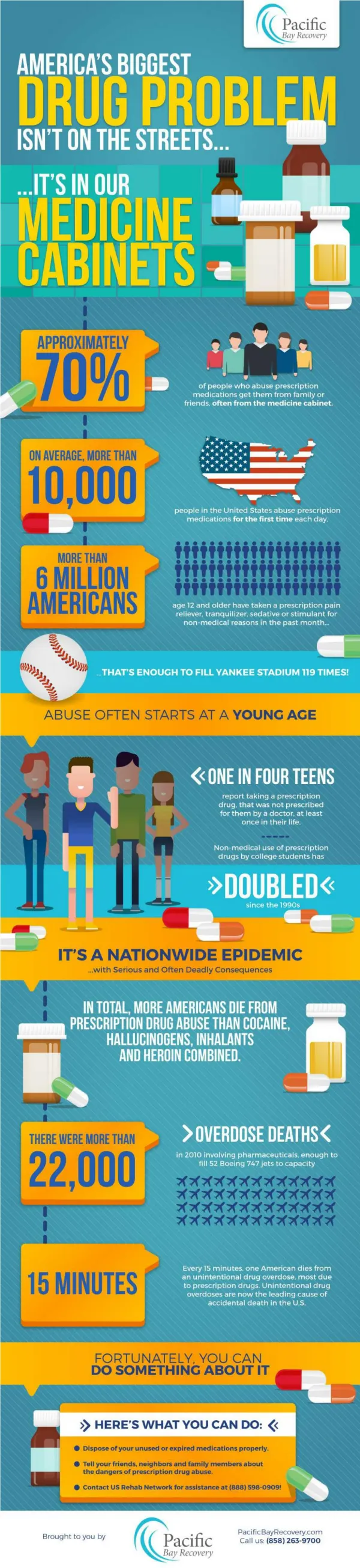
Consequences of “Better Pain Control” • Prescription drug abuse is the Nations fastest growing segment of drug abuse • CDC calls prescription drug abuse an “epidemic” • In 1999 fewer than 3000 prescription opioid deaths* • By 2008 there were nearly 15,000 opioid deaths* Office of National Drug Control Policy PaulozziPharmacoepidemiol Drug Saf. 2006;15:618-627 *National Vital Statistic Reports Vol 58 no 19;2010 *Paulozzi. MMWR, CDC Nov 1, 2011 vol 60
Results of Pain Aversive Culture • Prescription drug overdose is the second leading cause of injury death after car accidents nationwide • Deaths from prescription opiate overdose outnumber deaths from cocaine and heroine combined • Increased prevalence of pills available to the public • More interactions, abuse, diversion, addiction Warner et al. NCHS data brief #81. Natl Center for Health Statistics, 2011 Paulozzi. MMWR, CDC. Nov 1, 2011, vol 60
What this means for Oregon • Highest rate of prescription opiate abuse age 18-25 • Fifth highest overall rate of prescription opiate abuse • In past few years more Oregonians died of prescription overdoses than car accidents* • Substance abuse costs Oregon $5.9 billion/year** Oregon State Attorney General’s Office *CDC Natl Vital Statistics Reports Vol 58:19, 2007 **2009-2011 Domino Effect II Report, Legislative Assembly and Governors Council on Alcohol and Drug Abuse Programs
Pressure to Prescribe • We clinicians want to improve pain control • Federal recommendations to treat pain more aggressively • Federal reimbursement to be linked to satisfaction data • Without regard to outcome data or safety data • Increased direct consumer pharmaceutical marketing • Positive feedback cycle: More opiate use/dependence results in more specific requests for opiates • We prescribe more opiates now than ever before in history
American Culture • Americans are 4.6% of the worlds population • We consume 80% of the global opiate supply • We consume 99% of global hydromorphone • We consume 67% of worldwide illicit drugs • It is statistically impossible that we as a society have so much more pain than the rest of the world Paulozzi. MMWR. CDC. Nov 1, 2011, vol 60 USDOJ/DEA www.deadiversion.usdoj.gov/arcos/index.html
U.S. Opiate Sales • Opiate analgesic sales have quadrupled over the last decade (1999-2010) • Individuals with chronic pain have had a 740% increase in milligram morphine equivalents daily prescribed from 1997 to 2010 • This translates to an increase from 96 mg MSO4 equivalents/day to 710 mg MSO4 equivalents/day on average for each chronic pain sufferer Manchikanti. Pain Physician. 2008 Mar;11(2 suppl): S63-88
http://www.ncsl.org/issues-research/health/drug-overdose-death-rate-postcard.aspxhttp://www.ncsl.org/issues-research/health/drug-overdose-death-rate-postcard.aspx
Death rates parallel sales Source: National Vital Statistics System & Drug Enforcement Administration, ARCOS
Office of National Drug Control Policy, 2011 • Current Focus is on: • Education: directed at parents and youths • Dangers of abuse, proper storage and use • Monitoring: electronic monitoring programs • Disposal: develop drug disposal locations • Enforcement: improve law enforcement resources • Notably absent is physician education, awareness
State and Local Involvement • FDA proposes (REMS) Risk Evaluation and Mitigation Strategy • State Drug Prescription Monitoring Programs • Exist in 37 states. Established in Oregon 2011. • Specialty and State Consensus Guidelines • ACEP policy recommends judicious use of opiates and utilization of electronic drug monitoring programs DHHS, FDA Federal Register. Nov 7, 2011, 76. 68766-68767 ACEP Policy. Optimizing Pain… Ann Emerg Med. 2010;56:77-79 ACEP Policy. Electronic prescription monitoring. Ann Emerg Med. March 2012
The Buck Stops Here! • Each day nearly 100 Americans die from prescription opiate overdose • This is a 300% increase in the past 8 years • These medications are by prescription only • We are prescribing them • These deaths are iatrogenic • Not a single death has been attributed to pain US DHHS, CDC 2010 www.wonder.cdc.gov Natl Center Health Stats 2009 www.cdc.gov/nchs/data/databrifs/db22.htm
Impact on Public Health • 1.2 million Emergency visits due to misuse or abuse of prescription pharmaceuticals in 2009 • Compared to 1.0 million visits from illicit drugs • Increased ED utilization by 98.4% from 2004 • Prescription opiates are frequently diverted or sold for non-medical use by patients or their friends • Nonmedical use of opiates cost insurance $72.5 billion annually in health care costs www.oas.samhsa.gov/2k10/dawn034/edhighlights.htm www.oas.samhsa.gov/nsduh/2k9nsduh/2k9resultsp.pdf www.insurancefraud.org/downloads/drugDiversion.pdf
Here is the Challenge • Ensure the best quality of care for patients with pain • Balance “Do No Harm” with “Pain Control” • Do this in the greater context of epidemic prescription opiate abuse and overdose deaths • Challenge is to limit opportunities for abuse without reducing access for those in need of help • How can we do this?
How to control pain and manage an epidemic? • Utilize non-opiate adjuvants for pain • Talk with your patients about opiates • Hold your patients accountable for their medication • Reduce the overall number of pills available in society for diversion • Focus on Reasonable care!
Care Management Plans • Identify those with frequent needs • Identify cause of frequent needs • Develop Action Plan: Standardization • When and how to use urine screening • When and how to use pain contracts • Proper use of state drug monitoring programs • Criteria to decide how long patients should receive opioid analgesics • Criteria to decide when to refill or discontinue
Red Flags • Frequent or Recurrent visits with “pain” • Especially with negative findings • Allergy Lists • “Everything but” allergies • Allergy to Agonist/Antagonist • Pentazocine (Talwin), Butorphanol (Stadol), Buprenorphin (Subutex, Suboxone) • More concerned with Rx than Symptoms • Behavior out of proportion to exam findings
Physician Education • DEA Licensure is individual • Physicians choice in prescribing • Patients with objective painful findings deserve proper analgesia • Education to focus on “reasonable care” • Sprains, strains NSAIDS • Most non-cancer pain without clear objective findings should not receive opiates on initial presentation
Acute Back Pain • Proper HPI, Exam, Testing • NSAIDS • Muscle Relaxants • Steroids for radicular symptoms • Early activity/return to work • Physical therapy, ROM exercises, proper body mechanics • Avoid opiates for acute pain !
Opiates are detrimental • There exists a clear association between early opioid use (<6 weeks) for acute Low Back Pain and poor outcomes • Longer disability duration, higher medical costs • >8000 patients with 2 year follow up • Disabled 69 days longer, had 3 x increased surgery rate, had double the disability rate at 1 year • Authors conclude that “it is suggested that the use of opioids for the management of acute low back pain may be counterproductive to recovery” Spine 2007, Sept 1; 32(19):2127-2132.
Back Pain Guidelines • Medical workup seeking objective findings/etiology • Grade A recommendations (quality evidence) • Stay active, early return to work, APAP, NSAIDS • Grade B recommendations (some evidence) • Reassure, set expectations (90% improve in 6 wks) • Grade C recommendations (consensus, opinion) • Ice, topical NSAIDS, exercises J FamPract. 2009 Dec; 58(12):E1.
Acute Headache • What has been shown to reduce symptoms • NSAIDs, triptans, ergot alkaloids, compazine, barbiturates, opiates, parenteral medications • Marginal evidence • IV fluids, Steroids • What hasn’t been shown to help • Zofran, phenergan, reglan, benzodiazepines • Rebound headaches associated with opiates American Academy of Neurology, Headache Consortium, Guidelines
Acute Headache Treatment • Compazine 10 mg IV + Toradol 30 mg IV • Droperidol(Inapsine) 1.25 mg IV • Olanzepine (Zyprexa) 10 mg ODT • With single dose of PO Zyprexa 85% of severe headaches resolved in 1 hour AcadEmerg Med. 2008 Sept;15(9):806-811. J Emerg Med. 2011 Oct; 41(4):389-396.
Dental Pain • Multiple medical societies agree that Dental pain is best treated by a dentist! • PCN, clindamycin • NSAIDs • Nerve blocks are effective but short lived • Neuropathic agents may be attempted • Set limits on opiates if given! • Insist they see a dentist
Neuropathic Pain • Acute neuropathic radicular pain should receive an initial trial of steroids • Medrol dose pakand NSAIDS • With spasms? Add muscle relaxant • Most neuropathic medications are for chronic management and don’t work well for acute pain exacerbations • Gabapentin (Neurontin) • Pregabalin (Lyrica) • Venlafaxine (Effexor)
Neuropathic Pain • Opiates do not control neuropathic pain • Most reach critical sedation while still reporting uncontrolled pain • Try amitriptyline 25 mg PO for acute pain • May be prescribed as outpatient with qhs dosing • Avoid outpatient Rx in patients with overdose risk, depression, prior prescription misuse/abuse • Talk with patient about dangers of TCAs with overdose !
Acute Exacerbation of Chronic Pain • This is NOT considered to be ACUTE • This is a manifestation of chronic pain • Have you had this before, “Not like this!” • Some have “run out of medicines” • Not an Emergency, wont get a refill anymore • Personal responsibility (social not medical) • Most have “cabinet full of pills” • Try adjusting the existing medications
The IRON ED Institutional Reduction of Outpatient Narcotics from the Emergency Department • Letter mailed to all MDs to inform of new policy • ED will only treat ACUTE pain with outpatient Rx • Emphasis on primary provider as single point of ongoing narcotic access
Our Experience • 2 years of IRON ED • Press Ganey scores same or higher • ED MDs report greater job satisfaction • Less confrontation regarding prescriptions • Over 60% reduction in prescribed opiates