Download
1 / 1
10 likes | 142 Views
No. 088. Preliminary results of Robotic Assisted Laparoscopic Radical Prostatectomy following experience in Laparoscopic Radical Prostatectomy. Wolanski P*, Chabert C ¥# , Jones L ^ , Mullavey T ¥ , Walsh S † , Gianduzzo T ¥

E N D
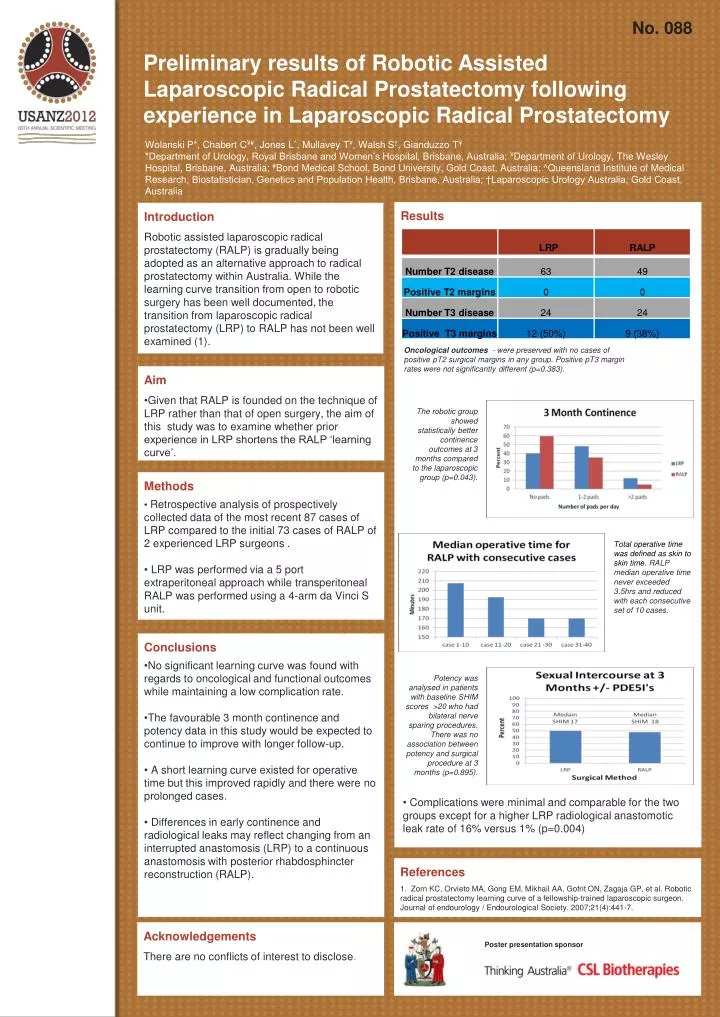
No. 088 Preliminary results of Robotic Assisted Laparoscopic Radical Prostatectomy following experience in Laparoscopic Radical Prostatectomy Wolanski P*, Chabert C¥#, Jones L^, Mullavey T¥, Walsh S†, Gianduzzo T¥ *Department of Urology, Royal Brisbane and Women’s Hospital, Brisbane, Australia; ¥Department of Urology, The Wesley Hospital, Brisbane, Australia; #Bond Medical School, Bond University, Gold Coast, Australia; ^Queensland Institute of Medical Research, Biostatistician, Genetics and Population Health, Brisbane, Australia; †Laparoscopic Urology Australia, Gold Coast, Australia Results Introduction Robotic assisted laparoscopic radical prostatectomy (RALP) is gradually being adopted as an alternative approach to radical prostatectomy within Australia. While the learning curve transition from open to robotic surgery has been well documented, the transition from laparoscopic radical prostatectomy (LRP) to RALP has not been well examined (1). • Oncological outcomes - were preserved with no cases of positive pT2 surgical margins in any group. Positive pT3 margin rates were not significantly different (p=0.383). • Aim • Given that RALP is founded on the technique of LRP rather than that of open surgery, the aim of this study was to examine whether prior experience in LRP shortens the RALP ‘learning curve’. The robotic group showed statistically better continence outcomes at 3 months compared to the laparoscopic group (p=0.043). • Methods • Retrospective analysis of prospectively collected data of the most recent 87 cases of LRP compared to the initial 73 cases of RALP of 2 experienced LRP surgeons . • LRP was performed via a 5 port extraperitoneal approach while transperitoneal RALP was performed using a 4-arm da Vinci S unit. Total operative time was defined as skin to skin time. RALP median operative time never exceeded 3.5hrs and reduced with each consecutive set of 10 cases. • Conclusions • No significant learning curve was found with regards to oncological and functional outcomes while maintaining a low complication rate. • The favourable 3 month continence and potency data in this study would be expected to continue to improve with longer follow-up. • A short learning curve existed for operative time but this improved rapidly and there were no prolonged cases. • Differences in early continence and radiological leaks may reflect changing from an interrupted anastomosis (LRP) to a continuous anastomosis with posterior rhabdosphincter reconstruction (RALP). Potency was analysed in patients with baseline SHIM scores >20 who had bilateral nerve sparing procedures. There was no association between potency and surgical procedure at 3 months (p=0.895). • Complications were minimal and comparable for the two groups except for a higher LRP radiological anastomotic leak rate of 16% versus 1% (p=0.004) References 1. Zorn KC, Orvieto MA, Gong EM, Mikhail AA, Gofrit ON, Zagaja GP, et al. Robotic radical prostatectomy learning curve of a fellowship-trained laparoscopic surgeon. Journal of endourology / Endourological Society. 2007;21(4):441-7. Acknowledgements There are no conflicts of interest to disclose. Poster presentation sponsor






