Download
1 / 26
260 likes | 509 Views
Differences in surgery regarding age. Findings: Acute Severe Pain Inflammation, swelling around the impacted or erupted tooth Trismus Traumatic ulceration Facial swelling Dysphasia Lymphadenopathy. Improvement. Extraction. Treatment: Irrigation Saline/h2O2 Debridement

E N D
Findings: Acute • Severe Pain • Inflammation, swelling • around the impacted • or erupted tooth • Trismus • Traumatic ulceration • Facial swelling • Dysphasia • Lymphadenopathy Improvement Extraction • Treatment: • Irrigation • Saline/h2O2 • Debridement • Analgesics • Mouth rinses • Antibiotics • Change • antibiotic • C&S • chlorhexidine • Hospitalize • (if facial • Infection) No Improvement Acute Types Pericoronitis Simple extraction Improvement Extraction Chronic • Findings: Chronic • Low grade • gingival • Inflammation • Asymptomatic • Treatment: • Irrigation • Saline/h2O2 • Debridement • Analgesics • Mouth rinses • Antibiotics? Improvement Difficult extraction
Pathobiology of OI Infections Environment is dominated by Anaerobes Micro-abscess formation Periapical infection Periodontal Infection Favorable Environment for Anaerobes Inoculation Into deep Tissues Liquefation necrosis Of tissues (collagenases) Metabolic by products (by streptococci) Abscess formation Synthesis of Hyaluronidase (Helps Infecting organisms to Spread) Breakdown of collagen Lysis of WBC Cellulitis
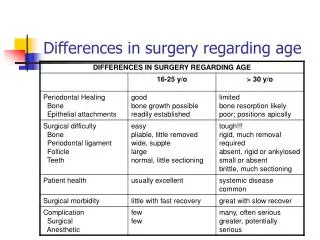
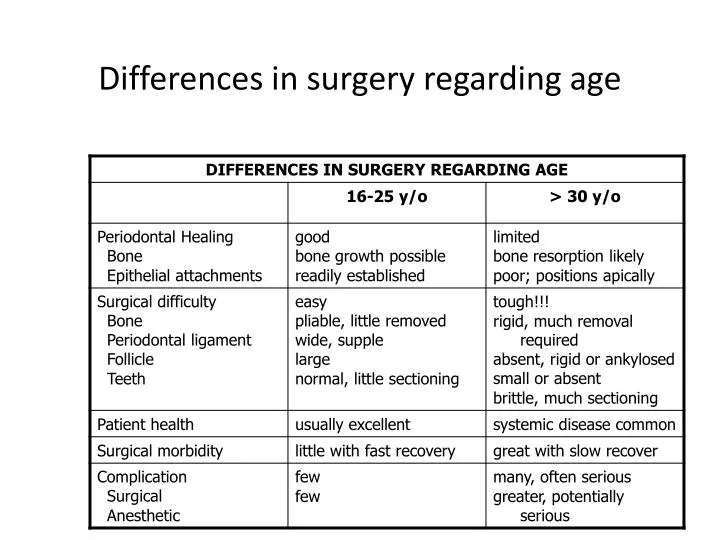
General differences between bone removal while extracting a root stump vs. impacted tooth
Post operative complications • Hemorrhage- Controlled by • Pressure gauze 15 minutes • Placement of gelfoam/sutures • Debridement of site with subsequent placement of gelfoam/sutures • Placement of surgicel (oxidized cellulose) • Topical thrombin with sutures, • Pressure!! • Pressure!!! • Further work-up may be indicated if above measures do not achieve adequate hemostasis.
PRINCIPLE1: Determine Severity of Infection PRINCIPLE2 : Evaluate state of Patient’s Host Defence Mechanisms PRINCIPLE 3: Treatment to be rendered by Generalist or OMF Surgeon PRINCIPLE4 :Treat Infection Surgically PRINCIPLE 5 : Support patient Medically PRINCIPLE 6 :Choose and Prescribe appropriate Antibiotic PRINCIPLE 7 : Administer Antibiotics Properly PRINCIPLE 8 : Post Operative evaluation Odontogenic Infections-Principles of therapy
Criteria for referral • Difficulty in breathing (________) (Remember the 4Ds) • Difficulty in swallowing(________) • Loss of fluids from the body(________) • Difficulty in opening the mouth(_______) • Swelling extending beyond the alveolar process • Elevated temperature (>101 F) • Severe malaise and toxic appearance • Compromised host defenses • Need for GA • Failed prior treatment
Management algorithm Discharge Treatment Secure Airway Incision & drainage Remove cause Culture and sensitivity Refer OMFS History/ Physical exam Pain Swelling Caries Pericoronitis Periodontitis Improvement 48-72 hours Assess severity Airway compromise Anatomic location Rate of progression Host defenses Immune status Medical co morbidities Systemic reserve Modify treatment Odontogenic Infection No improvement Re-evaluate Inadequate drainage Incorrect medication Other Foreign body Immune system compromise Imaging: PA Panoramic Look for Periapical Pathosis Impacted tooth Incision & drainage Remove cause Culture and sensitivity Out patient Procedure
Indications of Antibiotic Use • Temperature >101F with malaise • Spreading cellulitis • Chronic infection resistant to previous TX • Anatomical space involvement • Trismus • Lyphadenopathy • Pt with co-morbidities • Acute pericornitis, osteomyelitis, ANUG, etc…
Antibiotics Use Not Indicated • Minor, chronic, well localized abscess • Toothache • Periapical abscess • Dry socket • Multiple extractions in healthy patient • Surgical extraction (drill and sutures) • Mild pericoronitis • Drained alveolar abscess
Rational Antibiotic Therapy: • Is the ideal method for deciding on which antibiotic to administer, and is based on: • C&S of organisms involved • Site of infection • Safety of agent • Patients status • Cost of therapy
Empirical Antibiotic Therapy: • Broad-spectrum antimicrobials can be administered on a “educated guess” basis, considering: - Site of infection - Most probable pathogens - Antibiotic sensitivity pattern - C&S is not always cost and time effective
Mechanism of Action Classification • Eight Categories: • Blocks cell wall synthesis (inhibition of peptidoglycan cross-linking • Block peptidoglycan synthesis • Disrupt cell membrane • Block nucleotide synthesis • Block DNA topoisomerases • Block mRNA synthesis • Block protein synthesis (50S subunit) • Block protein synthesis (30S subunit)
Cell wall synthesis Cycloserine Vancomycin Bacitracin Penicillins Cephalosporins Monobactams 50S 50S 30S 30S Folic acid metabolism Trimethoprim Sulfonamides A T C DNA Protein synthesis (50S inhibitors) Erythromycin Chloramphenicol Clindamycin mRNA DNA-dependent RNA polymerase Rifampin Cell membrane Polymyxins DNA replication (DNA gyrase) Nalidixic acid Quinolones Protein synthesis (30S inhibitors) Tetracycline Spectinomycin Streptomycin Gentamicin, tobramycin Amikacin
Cefazolin Carbenicillin Imipenem/Cilastatin Cefadroxil Cephalexin Cephalothin Cephapirin Cephradine Cefamandole Cefaclor Ampicillin Cloxacillin Oxacillin Methicillin Penicillin V Penicillin G Amoxicillinn Cefoperazone Cefotaxime Ceftizoxime Ceftazidime Ceftibuten Ceftriaxone Moxalactam Cefixime Cefepime Cefdinir Cefuroxime Cefoxitin Cefotetan Cefmetazole Cefonicid INHIBITORS OF CELL WALL SYNTHESIS -LACTAMASE INHIBITORS Clavulanic acid Sulbactam -LACTAM ANTIBIOTICS OTHER ANTIBIOTICS Tazobactam Vancomycin Bacitracin PENICILLINS CEPHALOSPORINS CARBAPENEMS MONOBACTAMS Aztreonam 1st GENERATION 2nd GENERATION 3rd GENERATION 4th GENERATION
Stable to acid permitting oral administration Natural penicillins Penicillin G* Penicillin V Antistaphylococcal Cloxacillin Dicloxacillin Methicillin Nafcillin Oxacillin Amoxicillin + clavulanic acid Ampicillin + sulbactam Ticarcillin + clavulanic acid Piperacillin + tazobactam Stable to penicillinase Extended spectrum Ampicillin Amoxicillin Antipseudomonal Azlocillin Carbenicillin Mezlocillin Piperacillin Ticarcillin
Spaces of the Jaws • Deep Facial Spaces associated with any tooth • Vestibular • Subcutaneous • Buccal • Deep Facial Spaces associated with Maxillary teeth • Palatal • Infraorbital • Canine • Periorbital • Orbital • Cavernous Sinus • Deep Facial Spaces associated with Mandibular teeth • Space of the body of the mandible • Sublingual • Submandibular • Submental • Masticator • Submasseteric • Pterygomandibular • Superficial Temporal • Deep Temporal • Parotid
Buccal Space • Signs and symptoms • Cheek swelling (Below Zygomatic arch and above inf.border of Mandible) • Redness anterior to the masseter muscle • Can spread through subcutaneous tissues into the periorbital space • and past the inferior border of the mandible to the subcutaneous tissues lying superficial to the submandibular space.
Cavernous Sinus Thrombosis • Maxillary OI erode the Infra Orbital vein in the infra orbital space or the Inf Opthalmic vein via the sinuses • Follow Common Opthalmic vein through the superior ophthalmic fissure • Extends to Cavernous Sinus • Resulting inflammation caused by invading bacteria • Stimulates the clotting pathways • CS thrombosis