Download
1 / 25
260 likes | 305 Views
Learn about hemolytic anemias, disorders causing anemia due to premature red blood cell destruction. Explore classification, clinical features, laboratory evaluation, and manifestations. Understand acquired hemolytic anemias like autoimmune hemolytic anemia, its types, etiology, and clinical presentations. Discover the pathogenesis, diagnosis, and treatment options for various forms of hemolytic anemias.

E N D
Introduction toHemolytic Anemias Dr.Nisha Assistant professor Dept:of practice of medicine
HEMOLYTIC ANEMIAS Introduction • Definition • Classification • Pathogenisis • General clinical features • Laboratory evaluation of hemolysis
Hemolytic AnemiasDefinition • A group of disorders leading to anemia caused by a reduction in red cell life span. • RBC’s normally survive 60 - 120 days . • Bone marrow has the capacity to increase erythropoiesis 6 - 8 times than normal. • Anemia is the result of premature destruction of red cells exceeding the erythropoietic capacity of the bone marrow.
Hemolytic AnemiasClassification • Hemolytic anemias may be classified as I- Hereditary or acquired or II- Intracorpuscular or Extracorpuscular
Hemolysis may occur in two compartments I- Intravascular or II- Extravascular ( eg: spleen )
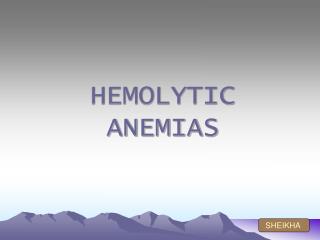
Red cell destruction Extravascular Intravascular Free plasma Hb Hpt and Hpx RES Hb Globin Haem+globin methem Haem Hb- Hpt complex Haemopexin-methem Excess Hb methaemalbumin Plasma protein pool Plasma iron pool Liver Protoporphyrin Unconjugated bilirubin Expired CO Kidney metHb Liver Hb Haemosiderin Conjugated bilirubin GI tract Urine Urobilinogen Faeces
Clinical Manifestations in Summary • Splenomegaly • Cholelithiasis(gall stones) symptoms • Leg ulcers (sickle cell, spherocytosis) • Skeletal abnormalities (thalassemia) • Crises (chronic hemolytic disease) • Aplastic crises (HPV-B19) • Hemolytic • Megaloblastic • Changes in urine color • Onset may be acute or insidious • Symptoms and signs of anemia • Jaundice • Acholuric • Without pruritus • Symptoms and signs specific to the type of hemolytic anemia • Symptoms related to the underlying disease
LABORATORY FİNDİNGSI-Increased RBC destruction • > 1 g /dl /week fall in blood Hb level* • Reduced glycosylated Hb • Signs of intravascular hemolysis • Hemoglobinemia* • Hemoglobinuria* • Hemosiderinuria* • Methemalbuminemia • Reduced serum hemopexin level • Decreased RBC life span • Increased haem(heme) catabolism • Increased serum unconjugated bilirubin* • Increased endogenous CO production • Increased urobilinogen excretion • Increased serum LDH* • Absence or decrease of serum haptoglobin*
LABORATORY FİNDİNGSII-Increased bone marrow activity and RBC production • Ferrokinetic • Increased plasma iron turnover • Increased RBC iron turnover • Biochemical • Increased RBC creatine • Increased activity of RBC enzymes eg: hexokinase, etc • Blood • Reticulocytosis • Macrocytosis • Polychromatophilia • Erythroblastosis • Leukocytosis and thrombocytosis • Bone marrow • Erythroid hyperplasia
Laboratory Evaluation of Hemolysis Intravascular Polychromatophilia Increased Erythroid hyperplasia unconjugated absent 0 + + ( severe cases) Extravascular Hematologic • Blood film Polychromatophilia • Reticulocyte Increased • Bone marrow Erythroid hyperplasia Plasma or serum • Bilirubin unconjugated • Haptoglobin , absent • Plasma free Hb N - • LDH Urine • Bilirubin 0 • Hemosiderin 0 • Hemoglobin 0 • Urobilinogen
Laboratory tests useful in differential diagnosis • Examination of peripheral blood • Special Lab. examinations
1.AUTOIMMUNE HEMOLYTIC ANEMIA • Auto antibodies(warm antibody- agglutinate the RBC at 37 C or cold antibody- agglutinate at lower temp,0 to 4 C) develop against the erythrocytes. • Warm antibodies generally belong to Ig G class,whereas cold antibodies are immunoglobuline M (Ig M). • In the warm antibody type,hemolysis takes place extravascularly in the spleen,while in the cold antibody type hemolysis occurs intravascularly or in the liver.
PATHOGENESIS • Antibody is usually of IgG class • Reacting with erythrocyte Rh antigen complex • Compliment activation may or may not occur • Antibody coated cells will be removed by the splenic macrophages • partially damaged erythrocytes may escape destruction • these repair themselves and appear as spherocytes.
CLINICAL FEATURES • Anemia • Jaundice • Splenomegaly • Acute Massive Hemolysis With Shock And Renal Failure
Hemolytic anemia of the cold antibody type may give rise to two clinical syndromes on exposure to cold environment. • Cold agglutinine syndrome • Paroxysmal cold hemoglobinuria
Cold agglutinine syndrome • Occurs in older patients,it presents with • acrocynosis • Raynaud’s phenominon • Gangrene of fingertips and • mild chronic hemolytic anemia
2.Paroxysmal cold hemoglobinuria • First identified auto immune disease described by Karl landsteiner,a pathologist from Vienna. • Antibody reacts with erythrocytes in the cold. • In PCH sudden hemolysis develops and leads to hemoglobinuria.
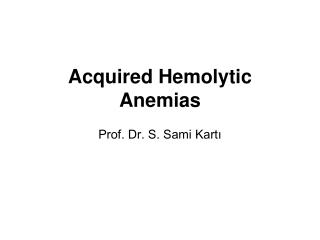
LAB INVESTIGATIONS in peripheral blood film shows • Marked anisopoikilocytosis • Polychromasia • Spherocytosis • Increase reticulocytes. • Neutrophil leukocytosis • Rarely platelets may be reduced due to development of antibodies against them(Evan’s syndrome)
anisopoikilocytosis polychromasia
The antibodies present on erythrocytes can be demonstrated by direct coomb’s test. • Free antibodies in the serum can be identified by the indirect coomb’s test.