Download
1 / 26
310 likes | 1.01k Views
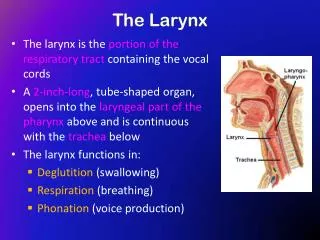
Chronic Infections of the Larynx. - Dr Subhodh H R. Chronic laryngitis Reinke’s edema Pachydermia larynges Atrophic laryngitis TB larynx Lupus of the larynx Syphilis of larynx Leprosy larynx Scleroma larynx. Chronic Hyperaemic laryngitis. Inflammation Without hyperplasia

E N D
Chronic Infections of the Larynx - Dr Subhodh H R
Chronic laryngitis • Reinke’sedema • Pachydermia larynges • Atrophic laryngitis • TB larynx • Lupus of the larynx • Syphilis of larynx • Leprosy larynx • Scleroma larynx
Chronic Hyperaemic laryngitis • Inflammation Without hyperplasia • Symmetrically involved inflammation of laryngeal subsites
Etiology • Following acute simple laryngitis • Other foci of head and neck infection. Eg: PNS, tonsils, teeth etc • Occupational factors. Eg: miners, strokers, gold & iron smiths, chemical factory workers • Smoking and alcohol • Chronic lung diseases • Vocal abuse
Clinical features • Hoarseness – commonest • Early fatigability of voice • Constant hawking • Discomfort in throat • Chronic cough • ILS : • Hyperaemia • Dull red and rounded cords • Flecks of viscid mucus on cords and inter-arytenoid region
Treatment • Eliminate other foci of infection • Avoid irritants ( smoking, alcohol, dust & fumes ) • Voice rest and speech therapy • Steam inhalation • Expectorants ( mucolytics )
Chronic hyperplastic laryngitis • Inflammation with hyperplasia • Maybe diffuse or localised • Localised variety presents as: dysphonia plica ventricularis, reinke’sedema, vocal nodules, vocal polyp, contact ulcer
Etiology: similar to Chronic hyperplastic laryngitis • Pathophysiology: • Begins in the glottis as hyperemia+edema and spreads around. • Mucosa, submucosa, glands, intrinsic muscles and joints are involved • Squamous metaplasia and hyperplasia with keratinisation • Mucous glands undergo hypertrophy initially and later atrophy
Clinical features • Predominantly Males • 30- 50yrs • Symptoms similar to chronic hyperaemic variety • ILS: • Dusky red mucosa and thickened. • Red swollen vocal cords, look irregular • Bulky false cords • Mobility maybe impaired due to oedema and infiltration, and muscle atrophy and CA joint arthritis.
Treatment • Conservative management as in Chr. Hyperaemic laryngitis • Surgical: • Vocal cord stripping – removing the hyperplastic mucosa • Damage to underlying vocal ligament be avoided • One side operated at a time
Reinke’s edema • Middle age • Bilateral symmetrical swelling of the membranous part of the vocal cords • Edema in the subepithelial space • Due to chronic irritation – voice misuse, smoking, LPR, chronic sinusitis, myxoedema
Clinical features: • Hoarseness – low pitched rough voice • ILS: • Fusiform appearance of the vocal cords with pale look • Hyperaemic and maybe hypertrophic false cords • Treatment: • Decortication of the vocal cords on one side and 3-4 weeks later on the other sides • Voice rest • Speech therapy
Pachydermia laryngis • Chronic hypertrophic laryngitis affecting the posterior part of larynx in the region of inter arytenoid and posterior part of the vocal cords
Cl/ F: • Husky voice • Irritation in the throat • ILS: • Red and grey granulation tissue in the inter arytenoid region and posterior thirds of the vocal cords • Contact ulcers • Bilaterally symmetrical • Treatment: • Microlaryngoscopic excision • Acid reflux treatment • Speech therapy
Atrophic laryngitis • Laryngitis sicca • Atrpohy of the laryngeal mucosa with crust formation • Common in women • Associated with atrophic rhinitis and pharyngitis
Cl/ f: • Intermittent hoarseness of voice due to crusts • Dry irritating cough • Occasional dyspnoea • ILS: • Atrophic mucosa • Foul smelling crusts • Excoriation and bleeding on removal of crusts • Maybe seen spreading along the trachea • Treatment: • Elimination of the cause • Humidification • Glucose in glycerine sprays • Expectorants
Tuberculosis of larynx • Almost always secondary to pulmonary TB • Middle aged males • Bronchogenic or haematogenic route of spread • Affects mainly posterior larynx: • Inter arytenoid fold • Ventricular bands • Vocal cords • epiglottis
Cl/f: • Weakness of voice • Hoarseness • Pain radiating to ears( ulceration ) • Dysphagia and odynophagia
ILS : • Hyperaemia with limited adduction • Mamillated inter arytenoid region • Mouse nibbled vocal cords ( ulceration ) and inter arytenoid regions • Granulation tissue • Turban epiglottis ( pseudoedema ) • Swollen false cords and AE folds • Surrounding pallor
Diagnosis: • X ray chest • Sputum examination • DL scopy biopsy • Treatment: • Voice rest • Anti TB drugs as for Pulmonary TB
Lupus larynx • Indolent tubercular infection associated with lupus of nose and pharynx • Involves the anterior part of the larynx • Epiglottis is commonly affected and maybe completely destroyed • Progresses downwards • Generally asymptomatic as it is painless • Diagnosed incidentally on routine examination in case of lupus of nose • Good prognosis with Anti TB drugs
Laryngeal syphilis • Rare • Gumma of tertiary stage maybe seen • May present as a smooth swelling which may ulcerate later • Diagnosis by biopsy and serology • Laryngeal stenosis may be a complication
Leprosy of the larynx • Rare • Associated with leprosy of nose and skin • Diffuse nodule over the epiglottis or AE fold or arytenoids • May ulcerate later • Diagnosis by biopsy • Deformity of the laryngeal inlet and stenosis are the complications
Scleroma larynx • Klebsiellarhinoscleromatis • Associated with nasal involvement • Smooth red swelling in the subglottis • Hoarseness, wheezing and dyspnoea • Diagnosis by biopsy • Treatment: • Streptomycin • Steroids • Subglottic stenosis is a complication