Download
1 / 1
10 likes | 185 Views
No. 089. A New Approach to Treating Lower Urinary Tract Symptoms When Medical Therapy Fails: The Prostatic Urethral Lift. Peter Chin a , Prem Rashid b , Damien Bolton c , Gregory Jack c , Anthony Ta c , Kevin Chu c , Jeffrey Thavaseelan d , Henry Woo e

E N D
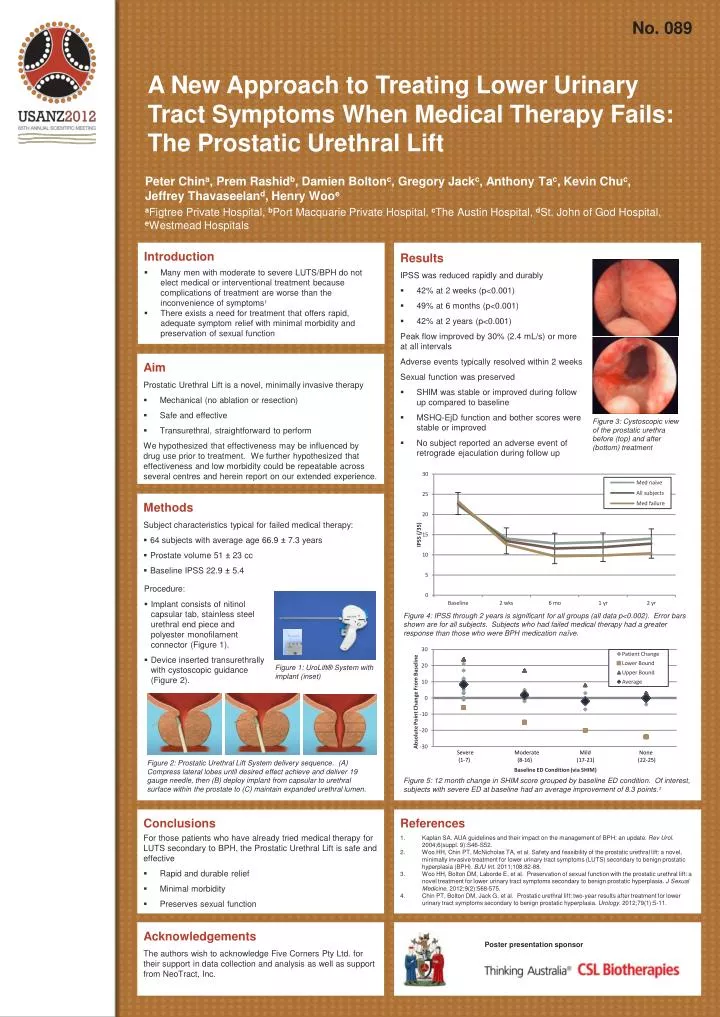
No. 089 A New Approach to Treating Lower Urinary Tract Symptoms When Medical Therapy Fails: The Prostatic Urethral Lift Peter China, PremRashidb, Damien Boltonc, Gregory Jackc, Anthony Tac, Kevin Chuc, Jeffrey Thavaseeland, Henry Wooe aFigtree Private Hospital, bPort Macquarie Private Hospital, cThe Austin Hospital, dSt. John of God Hospital, eWestmead Hospitals • Introduction • Many men with moderate to severe LUTS/BPH do not elect medical or interventional treatment because complications of treatment are worse than the inconvenience of symptoms1 • There exists a need for treatment that offers rapid, adequate symptom relief with minimal morbidity and preservation of sexual function Results • Results • IPSS was reduced rapidly and durably • 42% at 2 weeks (p<0.001) • 49% at 6 months (p<0.001) • 42% at 2 years (p<0.001) • Peak flow improved by 30% (2.4 mL/s) or more at all intervals • Adverse events typically resolved within 2 weeks • Sexual function was preserved • SHIM was stable or improved during follow up compared to baseline • MSHQ-EjD function and bother scores were stable or improved • No subject reported an adverse event of retrograde ejaculation during follow up • Aim • Prostatic Urethral Lift is a novel, minimally invasive therapy • Mechanical (no ablation or resection) • Safe and effective • Transurethral, straightforward to perform • We hypothesized that effectiveness may be influenced by drug use prior to treatment. We furtherhypothesized that effectiveness and low morbidity could be repeatable across several centres and herein report on our extended experience. Figure 3: Cystoscopic view of the prostatic urethra before (top) and after (bottom) treatment • Methods Subject characteristics typical for failed medical therapy: • 64 subjects with average age 66.9 ± 7.3 years • Prostate volume 51 ± 23 cc • Baseline IPSS 22.9± 5.4 • Procedure: • Implant consists of nitinol capsular tab, stainless steel urethral end piece and polyester monofilament connector (Figure 1). • Device inserted transurethrally with cystoscopic guidance (Figure 2). Figure 4: IPSS through 2 years is significant for all groups (all data p<0.002). Error bars shown are for all subjects. Subjects who had failed medical therapy had a greater response than those who were BPH medication naïve. Figure 1: UroLift® System with implant (inset) Figure 2: Prostatic Urethral Lift System delivery sequence. (A) Compress lateral lobes until desired effect achieve and deliver 19 gauge needle, then (B) deploy implant from capsular to urethral surface within the prostate to (C) maintain expanded urethral lumen. Figure 5: 12 month change in SHIM score grouped by baseline ED condition. Of interest, subjects with severe ED at baseline had an average improvement of 8.3 points.3 • Conclusions • For those patients who have already tried medical therapy for LUTS secondary to BPH, the Prostatic Urethral Lift is safe and effective • Rapid and durable relief • Minimal morbidity • Preserves sexual function References Kaplan SA. AUA guidelines and their impact on the management of BPH: an update. Rev Urol. 2004;6(suppl. 9):S46-S52. Woo HH, Chin PT, McNicholas TA, et al. Safety and feasibility of the prostatic urethral lift: a novel, minimally invasive treatment for lower urinary tract symptoms (LUTS) secondary to benign prostatic hyperplasia (BPH). BJU Int. 2011;108:82-88. Woo HH, Bolton DM, Laborde E, et al. Preservation of sexual function with the prostatic urethral lift: a novel treatment for lower urinary tract symptoms secondary to benign prostatic hyperplasia. J Sexual Medicine. 2012;9(2):568-575. Chin PT, Bolton DM, Jack G, et al. Prostatic urethral lift: two-year results after treatment for lower urinary tract symptoms secondary to benign prostatic hyperplasia. Urology. 2012;79(1):5-11. Acknowledgements The authors wish to acknowledge Five Corners Pty Ltd. for their support in data collection and analysis as well as support from NeoTract, Inc. Poster presentation sponsor