Download
1 / 82
830 likes | 1.07k Views
Risk factors for neonatal sepsis. Signs of sepsis In neonate. Maternal infections. 1 Syphillis: may pass through placenta may result in abortion, a stillborn, preterm labor or congenital syphillis (enlarged liver, spleen, skin lesions, rashes, oseteitis, pneumonia, hepatitis

E N D
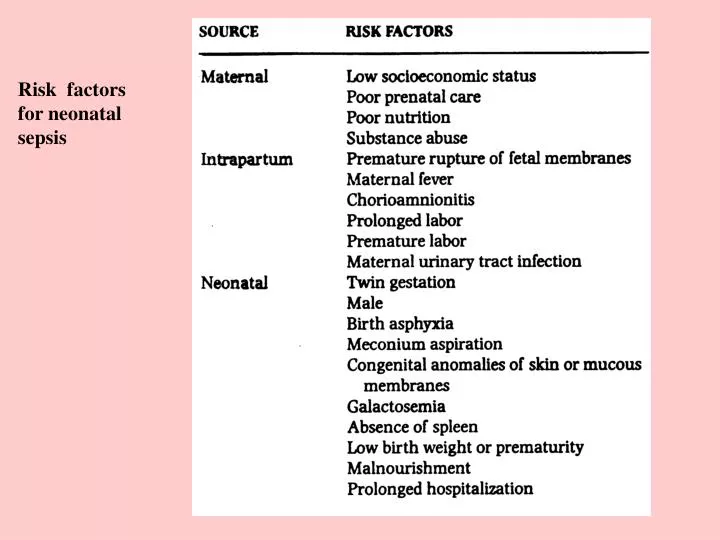
Risk factors for neonatal sepsis
Signs of sepsis In neonate
Maternal infections 1 Syphillis: may pass through placenta may result in abortion, a stillborn, preterm labor or congenital syphillis (enlarged liver, spleen, skin lesions, rashes, oseteitis, pneumonia, hepatitis TX penicillin 2 Chlamydial infection (#1 STD in US) : fetus may be infected during birth and suffer neonatal conjunctivitis or pneumonitis, which manifests at 4-6 wks of age PROM , chorioamnionitis, preterm labor TX erythromycin or amoxicillin (mom) 3 Gonarrhea: fetus may be infected during birth – ophthalmia neonatorium endocervicitis = PROM and preterm labor 4 Condyloma acuminatum or genital warts (human pailliomavirus): fetus may be infected during vaginal birth and develop epithelial tumors of the mucous membranes of the larynx in children. PG can cause proliferation HPV associated with cervical dysplasia & cancer (see next slide) 5 tichomoniasis basically associated with PROM and postpartum endometritis
Maternal vaginal infections Vaginal candidiasis: fetus may be infected during vaginal birth oral candidiasis (thrush) TX for infant Mycostatin TX for mom Monistat, Terazole, Femstat Most say treat for at least 7 days PROM, preterm labor, low birth weight, postpartum endometritis UTI’s , cycstitis, acute pyelonephritis PROM, preterm labor
Viral infections remember most virus passes placental barrier Cytomegalovirus: a member of herpesvirus group. Infects most humans peak ages 15 to 35 yrs. Like most herpes after primary infection, lies latent with periodic reactivation and shedding of the virus. Fetal & neonatal effects: 2% of all live births may be infected. These infants shed the virus from the nosopharynx and urine for several yrs. Most severe effects: deafness, mental retardation, seizures, blindness & dental bnormalities TX: gancyclovir for TX of congenitally infected infants No screening yet available Rubella: up to 10% of adults remain susceptible Fetal & neonatal effects: greatest risk is first 3 ms. 1/3 will result in spontaneous abortion, surviving maybe seriously compromised – deafness, mental retardaation, cataracts, cardiac defects, IUGR and mirocephaly. Infants will shed the virus for many months TX: prevention, A titer of 1.8 or greater provides immunity Rubella vaccine after delivery – educate no PG for at least 3 mos. WHY?
Rubella syndrome, or congenital rubella, is a group of physical abnormalities that have developed in an infant as a result of maternal infection and subsequent fetal infection with rubella virus. It is characterized by rash at birth, low birth weight, small head size, heart abnormalities, visual problems and bulging fontanelle.
Varicella – Zoster virus ( herpesvirus) = chickenpox: Acute infection for mom: r\preterm labor, encephalitis & varicella pneumonia. 5 –15% of aduls in US are susceptible Fetal & neonatal effects. Depend upon time of infection. If in the first 20 wks, the fetus may have congenital varicella syndrome (limb hypo- plasia, cutaneous scars, chorioretinitis, cataracts, microcephal and symmetric IUGR. In later pregnancy , transplacental passage of maternal antibodies usually protect fetus. However, the infant who is infected 4-6 days or 2 days after birth will not have the benefit of maternal antibodies, leaving the infant at risk for life-threatening neonatal varicella TX: immune testing, varicella-zoster immune globulin should be administered to women who have been exposed TX: infants born to mothers infected with varicella during the perinatal period, immunization with varicella-zoster immuni globulin as soon as possible but within 96 hrs after birth. Live attenuated vaccine after 12 mos through adults, avoid PG for 1 mo after each of the two injections, which are given 4 to 8 wks apart.
Herpesvirus serotypes 1 & 2: one of most common sexually transmissible disease. Most genital warts are type 2. Lesions form at site, begin at painful papules that progress to vesicles, shallow ulcers, pustules, crusts. Virus is shed until completely healed. lies latent in the sensory ganglion which can be reactivated Vertical transmission from mom to infant generally occurs: 1 after rupture of membranes or 2 during vaginal birth or with fetal scalp electrode Fetal & neonate effects: Primary infection in first 20 weeks : spontaneous abortion, IUGR and preterm labor. Neonatal herpes is uncommon but potentially devastating. From skin lesion to systemic or disseminated. If systemic death rate or serious sequelae is 50% . Watch for infection S&S temp instability, lethargy, poor sucking, jaundice, seizure & herpetic lesions. TX: no known cure although antiviral chemotherapy (acyclovir) Category C May breast feed if no lesions are on breast
Parvovirus: or erythemia infectiosum or fifth disease. highly communicable characterized by “slapped cheeks” appearance followed by a generalized maculopapular rash, fever, malaise and joint pain. Titers can be drawn if exposure during PG Fetal & neonate effects: I/4 to 1/3 of fetuses infected will have transient adverse effects, fetal death rate is less the 5%. Death usually results form failure of fetal RBC production, fetal anemia, hydrops (edema) and heart failure Hepatitis B : more likely to occur in person with STD, IV drug users & some population groups, Asians, Native Americans, Eskimos, Southeast Asian and subSaharan African immigrants. Chronic Hepatitis B develops in 1 to 6 % of infected adults who are at a greater risk for chronic liver disease, cirrohosis of the liver, premary hepatocellular carcinoma Fetal & neonatal effects: prematurity, low birth weight, and neonatal death increases. Infants born are chronic carriers of hepatitis B. Chronic hepatitis develops in about 90% of infected newborns – likely to have chronic liver disease
TX for Hepatitis B: prevention vaccines of 3 IM injections given during a 6 – 12 mos. period. Screen for HBsAg if at high risk screen again in 3rd trimester If mom is known GBsAg positive usually infection of the newborn can be prevented by administration of hepatitis B immune globulin followed by hepatitis B vaccine. Vaccine should be repeated at 1 and 6 mos. Breastfeeding is considered safe as long as the new born has been vaccinated HIV – human immunodeficiency virus. Fetal & neonatal effects: without prophylactic TX (Zidovudine) has a 20-30% of developing the disease. Typically are asysmptomatic at birth but S&S during first 12 mos. Enlargement of liver, spleen, lymphadenopathy, failure to thrive, persistent thrush, extensive seborrheic dermatitis or cradle cap. TX: prevention prenatal period intrapartum period (cesarean birth ? ) postpartum period (no breastfeeding) With Zidovudine throughout PG and L & D. infant TX with zidovudine syrup may test positive at birth but only 2% will remain positive If mom contacts HIV virus during PG higher change that infant will be HIV *
Non Viral infections: Toxoplasmosis: a protozoan infection. Raw or undercooked meat, cat feces crosses the placental barrier. Flu like symptoms in mom. Can do serologic test Fetal and neonatal effects: spontaneous abortion or live birth with congenital toxoplasmosis - 50% of infants. May be asymptomatic at birth or have low birth weight, enlarged liver and spleen, jaundice and anemia. Complications chorioretinitis or signs of neuologic damage may be several years later. TX: prevention and education Group B Streptococcus (GBS): is a leading cause of life threatening perinatal infections. 10 – 30% of women are colonized with GBS in the vaginal or rectal area. Most are asymptomatic or may include UTI, chorioamnionitis Fetal & neonatal effects: early onset GBS within 7 days of birth, usually 48 hrs. 1 – 2 % will develop early onset GBS, sepsis, pneumonia and meningitis. late onset is after the first week and meningitis is most common manifestation. Permanent neurological consequences may be seen in up to 50% of those who survive
Group B Streptococcus (GBS): is a leading cause of life threatening perinatal infections. 10 – 30% of women are colonized with GBS in the vaginal or rectal area. Most are asymptomatic or may include UTI, Chorioamnionitis Fetal & neonatal effects: early onset GBS within 7 days of birth, usually 48 hrs. 1–2 % will develop early onset GBS, sepsis, pneumonia and meningitis. late onset is after the first week and meningitis is most common manifestation. Permanent neurological consequences may be seen in up to 50% of those who survive TX: prevention, Cultures early and again at 35-37 wks. Intrapartum antibiotics, usually IV penicillin G 5 million units initially and 2.5 million units ever 4 hrs after until birth OR IV ampicillin, 2 g initially and 1g every 4 hrs until birth
Tuberculosis: Fetal & neonatal effects: perinatal infection is uncommon, may be acquired as a result of fetus aspirating amniotic fluid. Signs of congenital TB include TB failure to thrive, lethargy, respiratory distress, fever and enlargement of spleen, liver and lymph nodes. TX: for PG woman isoniazid, pyrazinamide and rifampin every day for 9 mos. Pyridoxine (vit B 6) should be given with isoniazid to prevent fetal nuerotoxicity. Some are using short term therapy – 1 to 2 months of therapy, and then twice weekly therapy TX for neonates. If mom’s sputum is free of organisms, infant does not need to be isolated from mom. Education is vital. Skin test of newborn – may be started on preventive isonaizid therapy. Skin testing again at 3-4 mos. If positive, receive isoniazid for at least 6 mos. If also have HIV should receive therapy for 12 mos. Breastfed infants of mothers taking isoniazid should receive pyridoxine with a multivitamin supplement
Potential Neonatal effects of maternal Cocaine use
Erythroblastosis fetalis, photomicrograph Antibodies from an Rh negative mother may enter the blood stream of her unborn Rh positive infant, damaging the red blood cells (RBCs). The infant responds by increasing RBC production and sending out immature RBCs that still have nuclei. This photograph shows normal RBCs, damaged RBCs, and immature RBCs that still contain nuclei.
erythroblastosis fetalis • "immune hydrops fetalis "hemolytic disease of the newborn" • lysis of fetal RBCs by maternal IgG antibodies • at risk: caucasians (15%); blacks (6%); Asians (1%) • findings: • anasarca (= skin edema) • fetal ascites • pleural effusion • increased diameter of umbilical vein • subcutaneous edema (skin thickness > 5mm) • polyhydraminos (75%) • placenatomegaly • pericardial effusion • hepatosplenomegaly
fetal hydrops • immune • Rh sensitization (erythroblastosis fetalis) • non-immune • thalassemia • structural defects (eg, lung tumor) • cardiac arrhythmia (2' to conduction defect) • U/S findings: • fetal ascites and/or pleural or pericardial effusion • subQ edema • polyhydramnosis • thick, hydropic placenta
Newborn jaundice (producing yellow skin) can have many causes, but the majority of these infants have a condition called physiological jaundice, a natural occurrence in the newborn due to the immature liver. This type of jaundice is short term, generally lasting only a few days. Jaundice should be evaluated by a physician until decreasing or normal levels of bilirubin are measured in the blood.
Less frequently, when neonatal jaundice is more severe, and ultraviolet light therapy is unable to break down all circulating bilirubin, exchange transfusion is often used. High levels of bilirubin in the blood can lead to brain damage and other serious problems. In these cases, exchange transfusion is a life-saving procedure designed to counteract the effects of serious jaundice, infection, or toxicity. The procedure involves the staged removal of the infant’s blood and replacement with fresh donor blood or plasma. • Guidelines for an exchange transfusion include: • hemolytic disease of the newborn (Rh disease) • life-threatening infection • severe disturbances in body chemistry • toxic effects of drugs • polycythemia
What should you protect & watch for? protect eyes skin watch for fluid volume deficit
Definition • ABO incompatibility can result when the fetal blood type differs from maternal blood type (that of the mother). • Causes and risks • A, B and O are the major blood types. ABO incompatibility between the mother and fetus can occur if: • the mother is O and the fetus is B or A or AB. (most common- represents almost 100% of the cases) • the mother is A and the fetus is B or AB (extremely uncommon) • the mother is B and the fetus is A or AB (extremely uncommon) • In these cases, the mother creates antibodies against the fetus’ incompatible blood type. These antibodies cross the placenta into the fetus’ blood stream where they begin to destroy the fetus’ blood cells. ABO incompatibility is similar to Rh incompatibility but generally creates much milder problems than Rh incompatibility. Newborn infants affected by ABO incompatibility may have elevated levels of bilirubin and become jaundiced (whites of the eyes and skin become yellow). Severe ABO incompatibility problems may require an exchange transfusion. However, most ABO incompatibility is relatively minor and the jaundice it produces can usually be treated with bili-lights (phototherapy).
What Are Neural Tube Defects (NTD's) • What are NTDs? • Neural tube defects, or NTDs, are birth defects that involve incomplete development of the neural tube, the structure that becomes the brain and spinal cord. There are several different types of NTDs. Spina Bifida and anencephaly comprise 90 percent of all NTDs. Encephalocele accounts for the remaining 10 percent. • Spina bifida is a birth defect of the spinal cord that is sometimes called "open spine." Spina bifida can range from a mild defect that causes no problems, to a serious condition involving muscle paralysis, loss of feeling, infection and loss of bowel and bladder control. Spina Bifida is the leading cause of childhood paralysis in the U.S. • Anencephaly is a birth defect resulting in babies being born with underdeveloped brains and incomplete skulls. Most babies born with anencephaly do not survive more than a few hours after birth. • Encephalocele is a birth defect that results in a hole in the skull through which brain tissue protrudes. Babies with encephalocele usually live but they often suffer varying degrees of mental disability
When and why do NTDs happen? • NTDs occur very early in a baby’s development, between the 17th and 30th day after conception. In addition to folic acid deficiency, other factors such as environment, genetics, maternal diabetes, and socioeconomic status may play a role. • How many pregnancies are affected by these birth defects? • In the United States, about 4,000 pregnancies per year are affected by an NTD. Of these, about 1,500 pregnancies result in miscarriage or stillbirth. About 2,500 babies (about 1 in 1,000) in the United States are born with an NTD each year. • Who is at risk of having a baby with an NTD? • Any woman can have a baby with an NTD. At particular risk are women who: • Are of Hispanic ethnicity • Have diabetes • Use valproic acid or carbamazepine to treat seizure disorders • Have an NTD themselves or have a close relative with one • A woman who has had a previous NTD-affected pregnancy is at increased risk of having another such pregnancy. She should consult her doctor before her next pregnancy about the amount of folic acid she should take. Studies have shown that a larger dose of folic acid ¾ 4.0 milligrams (4,000 micrograms) beginning at least one month before pregnancy and through the first trimester reduces the risk of having another affected pregnancy by about 70 percent.
What is Anencephaly?Anencephaly is a neural tube defect (a disorder involving incomplete development of the brain, spinal cord, and/or their protective coverings). The neural tube is a narrow sheath that folds and closes between the 3rd and 4th weeks of pregnancy to form the brain and spinal cord of the embryo. Anencephaly occurs when the "cephalic" or head end of the neural tube fails to close, resulting in the absence of a major portion of the brain, skull, and scalp. Infants with this disorder are born without both a forebrain (the front part of the brain) and a cerebrum (the thinking and coordinating area of the brain). The remaining brain tissue is often exposed--not covered by bone or skin. The infant is usually blind, deaf, unconscious, and unable to feel pain. Although some individuals with anencephaly may be born with a rudimentary brain stem, the lack of a functioning cerebrum permanently rules out the possibility of ever gaining consciousness. Reflex actions such as respiration (breathing) and responses to sound or touch may occur. The cause of anencephaly is unknown. Although it is believed that the mother's diet and vitamin intake may play a role, scientists believe that many other factors are also involved. Is there any treatment?There is no cure or standard treatment for anencephaly. Treatment is supportive. What is the prognosis?The prognosis for individuals with anencephaly is extremely poor. If the infant is not stillborn, then he or she will usually die within a few hours or days after birth. What research is being done?The NINDS conducts and supports a wide range of studies that explore the complex mechanisms of normal brain development. The knowledge gained from these fundamental studies provides the foundation for understanding how this process can go awry and, thus, offers hope for new means to treat and prevent congenital brain disorders including neural tube defects such as anencephaly
What are Encephaloceles?Encephaloceles are rare neural tube defects characterized by sac-like protrusions of the meninges (the membranes that cover the brain) and brain tissue through abnormal openings in the skull. The defects are caused by failure of the neural tube to close during the development of the fetus. Symptoms may include hydrocephalus, spastic quadriplegia (paralysis of all 4 limbs), developmental delay, microcephaly, vision problems, mental and growth retardation, ataxia, and seizures. Some affected children may have normal intelligence. Encephaloceles are often accompanied by craniofacial abnormalities or other brain malformations. Is there any treatment?Generally, surgery is performed during infancy to place the protruding tissues back into the skull, remove the sac, and correct the associated craniofacial abnormalities. Hydrocephalus may require a shunt. Other treatment is symptomatic and supportive. What is the prognosis?The prognosis for individuals with encephaloceles varies depending on what brain tissue is involved, the location of the sacs, and the accompanying brain malformations. What research is being done?The NINDS conducts and supports a wide range of studies that explore the complex mechanisms of normal brain development. The knowledge gained from these fundamental studies provides the foundation for understanding how this process can go awry and, thus, offers hope for new means to treat and prevent congenital brain disorders including neural tube defects such as encephaloceles
The rate of spina bifida in 1999 was 20.83 per 100,000 live births. The rate has declined significantly between 1995 and 1999. In 1999, 735 cases of spina bifida were reported. After a decline in the early part of the decade, the anencephalus rate has been stable since 1994. The rate of anencephalus in 1999 was 10.57 per 100,000 live births. There were 373 reports of anencephalus in 1999. Birth certificate data for 1991-98 are final, but data for 1999 are preliminary. The preliminary birth data used here are 97.6% complete. The numbers and rates for all years exclude data for Maryland, New Mexico, and New York, which in various years had either incomplete reporting or did not report these neural tube defects. Both spina bifida and anencephalus are considered underreported on the birth certificate. CDC is continuing to monitor and analyze neural tube defect occurrence data.
Ventricles of brain Cerebrospinal Fluid (CSF) is a clear, water-like fluid produced primarily within the lateral ventricles of the brain. In each ventricle, small flower-like tufts called choroid plexus produce CSF at a constant rate. The fluid flows through a discrete channel into the space around the brain and spinal cord, where it also functions as a cushion, and it is reabsorbed back into the blood stream. A small amount of CSF is also produced by the spinal cord. The CSF contains important chemicals and carries waste products away from tissues in and around the brain. Hydrocephalus occurs when CSF accumulates as a result of a blockage in the circulation path or an overproduction. The total volume of CSF is 125-150 ml. The normal resting pressure of the CSF is between 150-180 mm H2O. It has been calculated that 430 to 450 ml of CSF are produced every day.
Treatment by shunting the cerebrospinal fluid (CSF) to another area of the body, generally allows patients to lead full and active lives. There are different kinds and models of shunting systems. Although, shunts were a major medical breakthrough, there are problems that still remain unsolved in the treatment of hydrocephalus, such as shunt obstruction and infection.An overwhelming majority of newborns with hydrocephalus will have a normal life span and normal or even superior intelligence. In addition, they will enjoy normal activities and be useful members of society. However, there are complications associated with hydrocephalus with learning disabilities being one of the most prevalent.In most cases, hydrocephalus is not hereditary.
Types of HydrocephalusHydrocephalus is a condition that can exist during one of two stages. It can be congenital, when the condition exists at birth or acquired, when it occurs as the result of a trauma to the brain after birth. Forms of HydrocephalusHydrocephalus exists in two forms; communicating (non-obstructive hydrocephalus) caused by inadequate absorption of CSF when the ventricular pathways are not obstructed or noncommunicating (obstructive hydrocephalus) caused by blockage in the ventricular pathways through which CSF flows