Download
1 / 63
660 likes | 847 Views
Telemedicine: Transforming the Delivery of Healthcare. Debbie Voyles, MBA HOM Director of Telemedicine F. Marie Hall Institute for Rural and Community Health June 2013. Texas Tech University Health Sciences Center F. Marie Hall Institute for Rural and Community Health. Five Core Programs

E N D
Telemedicine: Transforming the Delivery of Healthcare Debbie Voyles, MBA HOM Director of Telemedicine F. Marie Hall Institute for Rural and Community Health June 2013
Texas Tech University Health Sciences CenterF. Marie Hall Institute for Rural and Community Health • Five Core Programs • Telemedicine –community-based telemedicine in Texas; one of 2 correctional programs; one of longest running programs in nation; 45,000+ consultations • TexLa Telehealth Resource Center • Rural Research – Project FRONTIER, TARC, Alzheimer’s Disease • Health Education – West Texas Area Health Education Center (WTAHEC), Hot Jobs, Double-T Health Service Corps, region-wide community health needs assessment • Electronic Health Records – West Texas Health Information Technology Regional Extension Center (WTxHITREC)
Today’s Discussions: • Unique challenges for Rural Health Care • What is Telemedicine • Benefits to using Telemedicine • Challenges/Barriers to Telemedicine • Critical Steps to Implement Telemedicine • Reimbursement • TexLa Telehealth Resource Center
US 2010 Census • Population = 308,745,538 • 9.7% increase from 2000 • 83.7% live in the nations 366 metro areas (population over 50K) • 10.0% live in the nations 576 micro areas (population between 10K and 50K) • 6.3% live in rural areas (population less than 10K) US Department of Commerce Population Distribution and Change: 2000 to 2010
Current Challenges in Rural Health Care • Workforce shortages • Geographic isolation – limited transportation • Diminishing community economics • Low healthcare margins • Difficulty recruiting physicians • Increasing dependence on specialty and expensive technologies • Demand for quality
Lipscomb Dallam Sherman Hansford Ochiltree Hartley Hutchinson Moore Roberts Hemphill Oldham Potter Carson Gray Wheeler Collings- worth Deaf Smith Randall Armstrong Donley Parmer Castro Swisher Briscoe Hall Childress Hardeman Cottle Motley Wilbarger Hale Floyd Bailey Lamb Wichita Foard Clay Montague Lamar Cooke Grayson Red River King Baylor Crosby Dickens Archer Lubbock Cochran Hockley Knox Fannin Bowie Delta Jack Titus Wise Denton Collin Garza Kent Lynn Stonewall Haskell Throckmorton Young Terry Franklin Yoakum Hopkins Hunt Morris Cass Camp Rockwall Rains Tarrant Marion Wood Parker Dallas Palo Pinto Borden Scurry Gaines Dawson Fisher Jones Shackelford Stephens Upshur Kaufman Van Zandt Harrison Gregg Hood Johnson Smith Ellis Eastland Howard Andrews Martin Mitchell Nolan Taylor Callahan Erath Somervell Henderson Panola Rusk Navarro Hill Comanche Bosque Coke Ector Midland Glasscock Winkler Loving Cherokee Sterling Runnels Anderson Shelby Coleman Brown El Paso Hamilton Freestone Nacogdoches McLennan Limestone Ward Mills Hudspeth Culberson Crane Tom Green San Augustine Coryell Upton Reagan Sabine Concho Reeves Houston Irion Leon Angelina Falls McCulloch Lampasas San Saba Trinity Bell Robertson Madison Schleicher Menard Polk Burnet Milam Newton Pecos Tyler Jasper Walker Crockett Mason Jeff Davis Llano Brazos Williamson San Jacinto Grimes Sutton Burleson Kimble Travis Hardin Gillespie Lee Montgomery Blanco Terrell Washington Liberty Orange Bastrop Kerr Hays Waller Presidio Edwards Kendall Val Verde Austin Jefferson Fayette Harris Caldwell Real Brewster Comal Bandera Chambers Colorado Guadalupe Fort Bend Gonzales Bexar Lavaca Galveston Uvalde Medina Kinney Wharton Brazoria Wilson De Witt Jackson Karnes Atascosa Zavala Frio Matagorda Victoria Maverick Goliad Calhoun Dimmit Bee McMullen Live Oak La Salle Refugio Aransas San Patricio Webb Nueces Jim Wells Duval Kleberg Jim Hogg Brooks Zapata Kenedy Starr Willacy Hidalgo Cameron Texas Counties Without a Pharmacists Source: Texas Department of Rural Affairs, August 2010
Presidio, TX ACCESS Hospital: Clinics: Physicians: Nurses: P.A.s: 0 1 1 2 .5 Population: Medicaid Enrolled: 4167 705 (nearest 85mi.) El Paso to Lubbock: 343 mi. / 7 hrs. Presidio to Lubbock: 398 mi. / 7.5 hrs.
Could healthcare be better? • If it were available anywhere at anytime to anyone • Costs were reduced and outcomes improved • Practitioners could consult with experts and each other anytime and anywhere • Chronically ill and homebound patients could be monitored remotely 24/7/365 • Preventive care could be integrated into work, home, school, or any environment With Telemedicine it is possible!
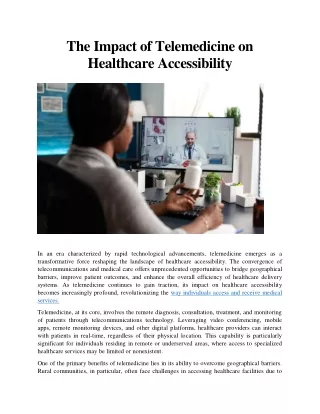
What is Telemedicine?American Telemedicine Association • It the use of medical information exchanged from one site to another via electronic communications to improve patients’ health status. • It has evolved to telehealth to incorporate health education, prevention and anticipatory guidance that does not always involve clinical services • It may include videoconferencing, transmission of images, e-health, m-health, patient portals, remote monitoring of clinical information, etc. • It is not a separate medical specialty!
Three Links to Effective Telemedicine Technology Specialized Care Provider Patient
How can Telehealth/Telemedicine be used? • “Shrinking the distance” • Increasing access • Bridging the gaps • Serving the needs • “Care closest to home” • Medically underserved rural areas • Health professions shortage areas • Saves travel time / increases convenience • Lowers costs • Aging & chronic conditions • Special populations (Prisons) • Disaster response & relief efforts • Refocus on prevention, team-based community-centric care
How it Works • Video conference system (SF & RT) • Various medical peripherals (heart rate, blood pressure, ekg, dematomes, otoscopes, etc.) • Connectivity (High-speed T-1 phone lines, DSL, Wireless, Satellite, Cloud, etc.) • Consultant – physician or specialists • Presenter – in Texas any certified healthcare provider working within the scope of their license
Telemedicine Components • Equipment standardization • Peripherals • Otoscope • General Exam Camera • Dermatology • Burn Care • Wound Care • Stethoscope Color Printer
Service Lines • Burn/Wound Care • Dermatology • Genetics • Infectious Disease • Mental Health • Neurology • Nutritional • Orthopedics • Primary Care • Pulmonology • Cardiology • Endocrinology • Geriatrics • Internal Medicine • Nephrology • Oncology/Hematology • Pharmacy • Pulmonology • Urology
Telemedicine Philosophy • Telemedicine does not alter the practice of medicine. • It is only a tool.
Telemedicine Access • Response to: • Fewer physicians in rural/frontier communities • Fewer specialists throughout region • Technology advancements • Changes to state rules • Services w/out taking too much time off from work/school • Reduces escalating (spiking) personal travel costs • Another way to see a health care professional; comparable to face-to-face care… • Meeting increasing need for specialties due to increasing chronic illnesses (diabetes, obesity, psychiatric, geriatric, cognitive…) • Expand benefits that health services bring to rural and frontier communities • …and patients like telemedicine
Benefits to Using Telemedicine • Improved access to specialty services and care – “care closest to home” • High patient satisfaction – • improved access, • reduced travel costs (mileage and travel time) • reduced time away from home/school/work • Improved patient outcomes – earlier interventions, reduced complications, consistent use of evidenced based medicine • Healthy People/Healthy Communities - better relationships with rural communities – create, improve and maintain local access to appropriate high quality care
Challenges/Barriers to Telemedicine • Keeping up with changes in technology • Investment in equipment and training • Credentialing/licensing (especially across state lines) • Limits on reimbursement from insurance companies, Medicare, Medicaid • Connectivity issues • Regulatory Restrictions • Systems implementation and interoperability • End user adoption and training
Critical Steps to Implementation • Community Assessment – in person • Be clear on goals – what are you trying to achieve? • Identify a telemedicine team – find champions • Determine how telemedicine will fit into the organizational structure • Develop a plan for educating and training • Continually educate senior leadership, medical staff, community and state leaders, on performance and advances
Treat Telemedicine The Same As Any Other Practice of Medicine • Apply same protocols, techniques, standards and style • Treat patient in the same manner as if they were presented in the same room
Licensure • State licensing – does not require a different license • Physician must be licensed in the same state the patient is located • Federal licensing proposal
Telemedicine Credentialing and Privileging Requirements If seeing patients in a hospital setting must be credentialed with facility as if seeing the patient in person New CMS rule, which applies to all hospitals that participate in Medicare, and inpatients at critical access hospitals, upholds The Joint Commission's current practice of allowing the hospital or CAH to utilize information from the distant-site hospital or other accredited telemedicine entity when making credentialing or privileging decisions for the distant-site physicians and practitioners.Effective July 5, 2011
Confidentiality and Consent Forms • Employee confidentiality forms • Patient consent to treatment form – same as if being seen face to face • Release of medical records forms
Telemedicine Reimbursement • Medicare • Medicaid • Third-Party • Private Pay
Medicare • Eligible areas include: • Health Professional Shortage Area (HPSA) • County that is not included in metropolitan statistical area (MSA) • Eligible sites include: • Office of physician or practitioner • Critical access hospital (CAH) • Rural health clinic (RHC) • Federally qualified health clinic (FQHC) • Hospital • Skilled nursing facility (SNF) • Hospital-based or CAH-based Renal Dialysis Centers (including satellites) • Community mental health center (CMHC)
Medicare • Practitioner who may bill: • Physician • Nurse practitioner (NP) • Physician assistant (PA) • Nurse midwife • Clinical nurse specialist (CNS) • Clinical psychologist (CP) and clinical social workers (CSW) (CPs and CSWs cannot bill for psychotherapy services that include medical evaluation and management services under Medicare. These practitioners may not bill or receive payment for Current Procedural Terminology (CPT) codes 90805, 90807, and 90809) • Registered dietitians or nutrition professionals
Medicare – Eligible Medical Services • Office or other outpatient visits (99201-99215) • Individual psychotherapy (90804-90809) • Pharmacologic management (90862) • Psychiatric diagnostic interview examination (90801) • End stage renal disease related services included in the monthly capitation payment (90951, 90952, 90954, 90955, 90957, 90958, 90960 and 90961) • Individual Medical Nutritional Therapy (G0270, and 97802-97804) • Individual and group diabetes self-management training services (G0108-G0109) • Neurobehavioral status examination (96116)
Medicare – Eligible Medical Services • Individual and group health and behavior assessment and intervention (96150-96154) • Follow-up inpatient Telehealth consultations (G0406, G0407 and G0408) • Emergency department or initial inpatient telehealth consultations in hospitals and SNFs (G0425-G0427) • Subsequent hospital care services (but not more frequently than once every 3 days) (99231-99233) • Subsequent nursing facility care services (but not more frequently than once every 30 days) (99307-99310) • Individual and group kidney disease education services (G0420-G0421) • Smoking cessation services (99406-99407, G0436-G0437)
Medicare – New for 2013 • 7/30/12 Proposed Rule to add two codes for “alcohol and/or substance abuse (other than tobacco) structured screening (e.g. AUDIT, DAST) and intervention services” • (G-0396 – 15-30, • G0397 – more than 30 minutes) • (NOTE: not screening services but as part of diagnosis or treatment of an illness or injury) • Preventive Services added in 2012 now available. • G0442-G0443. Annual alcohol misuse screening and counseling, • G0444 Annual depression screening, • G0445 Screening for sexually transmitted infections and counseling, • G0446 Intensive behavioral therapy for cardiovascular disease • G0447 Intensive behavioral therapy for obesity
Medicare • Distant site physicians and practitioners submit claims for Telehealth services using the appropriate CPT or HCPCS code for the professional service along with the Telehealth modifier GT, “via interactive audio and video telecommunications system.
Medicare • Originating sites are paid an originating site facility fee HCPCS Code Q3014. The originating site facility fee is a separately billable Part B payment. • Current fee is $24.24
Telemedicine Reimbursement Medicaid • 35 States Reimburse for Telemedicine • Alabama, Alaska, Arizona, Arkansas, California, Colorado, Georgia, Hawaii, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maine, Michigan, Minnesota, Missouri, Montana, Nebraska, Nevada, North Carolina, North Dakota, Oklahoma, Oregon, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, Wyoming
Texas Medicaid Reimbursement • Current Texas Medicaid • Started reimbursing in 1998 • One of the first states in the country • Must be “face to face” interactive video, no store and forward, except for Tele-radiology • Patient site bills for a facility fee – • Code Q3014 • Must use GT modifier, indicating it was a telemedicine visit