Download
1 / 21
220 likes | 262 Views
Learn about multi-organ dysfunction in ICU, indicators of organ failure, causes of MODS, management strategies, supportive measures, and specific organ support techniques to improve patient outcomes. Understand complications of prolonged ICU stay and the prognosis of organ failure.

E N D
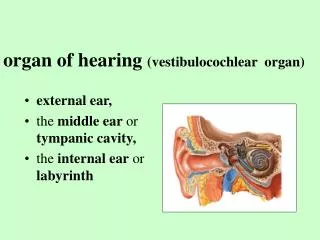
Organ failure in ICU • Can be a consequence of direct injury (eg pneumonia/MI/toxin) • Can also occur as a consequence of shock with tissue ischaemia and dysfunction occurring as a consequence of hypoxia.
Indicators of organ failure Respiratory – Requiring supplementary oxygen +/- ventilation Cardiovascular - Low blood pressure or on vasopressors/inotropes Renal – reduced or no urine output, raised serum creatinine Nervous System – Reduced conscious level Liver – Coagulopathy, low blood sugar, high lactate, encephalopathy, raised bilirubin (without other cause) Haematological – Low platelets, deranged coagulation tests (e.g. prothrombin time)
Multi-Organ Dysfunction Syndrome (MODS) is the term used to describe loss of physiologic reserve and progressive organ injury associated with critical illness.
Multiple Organ Dysfunction Syndrome • Shock causes hypoperfusion, lack of oxygen at a cellular level then leads to cellular dysfunction/death • Cellular dysfunction/death causes release of inflammatory cytokines and microvascular injury • This cascade then causes further cellular dysfunction and whole organ system failure ensues
Management of MODS • Treat the underlying cause! • Supportive: • Oxygenation, ventilation • Fluid/Inotropes/vasopressors • Feeding • Replacement • Mechanical organ specific support (renal replacement therapy, extracorporeal hepatic support, Left-ventricular support, ECMO) • Avoid the complications of prolonged ICU stay
General Supportive Measures • Feeding • Sedation and Invasive ventilation • Gastric protection • DVT prevention • Measures to limit nosocomial infection • Analgaesia
Specific Organ Support- Respiratory • Non Invasive Ventillation • BIPAP & CPAP • See subsequent respiratory lecture
Specific Organ Support- Respiratory • Respiratory • Intermittent Positive Pressure Ventilation • Pressure support ventilation • Tracheostomy • Slow weaning of ventilatory support
Specific Organ Support –ECMO • Extracorporeal Membrane Oxygentaion • Only used in acute, severe REVERSIBLE respiratory or cardiac failure, with a high risk of death, that is refractory to conventional management. • Only available in certain specialist centres • Blood is removed from the body, oxygenated by a machine, then returned. • Frequent and severe complications
Specific Organ Support- Cardiovascular • Limited options • Vasoactive agents • Intra-aortic balloon pump
Specific Organ Support- Renal • Renal failure is common and is often reversible when it occurs as a consequence of MODS • Renal replacement therapy involves mechanical replacement of renal function (essentially a ‘kidney machine’ .
Indications to commence Renal Replacement Therapy • Symptomatic uraemia (encephalopathy, pericarditis, bleeding) • Fluid overload • Metabolic acidosis due to renal failure • Resistant hyperkalaemia • Non-renal • certain toxins/drugs • resistant hypernatraemia • temperature control • removal of inflammatory cytokines (no evidence-controversial)
Types of Organ Support • Renal – provide a temporary means of filtering or dialysing the blood in patients with renal failure (CVVHDF)
Types of Organ Support • Nervous system – a patient may need to be sedated (and thus intubated and ventilated): • or their own safety e.g. if encephalopathic • if they have a reduced GCS and may not be able to protect their own airway. • Temperature management post cardiac arrest • If they have a brain injury
Complications of prolonged ICU stay • Ventilator-associated pneumonia • Vascular catheter associated bloodstream infection • Catheter-associated urinary tract infection • Venous thromboembolism • ICU acquired weakness • Paralytic ileus • Ischaemia from arterial lines • Stress ulcers • Psychological sequelae and cognitive dysfunction
Prognosis in organ failure • Mortality ranges from 30% to 100% where mortality increases as the number of organs involved increases Mortality Number of organ systems involved
Summary • Multi-organ Dysfunction can be avoided by prompt treatment of shock and its causes. • Low urine output can be the first sign of organ dysfunction • Organ support has many complications • Multi-organ failure carries a high mortality