Download
1 / 35
490 likes | 2.11k Views
Bacteremia. MLAB 2434 –Microbiology Keri Brophy-Martinez. Definitions. Pseudobacteremia False bacteremia Contamination of a blood culture during or after collection. Definitions. Bacteremia – presence of bacteria in blood stream

E N D
Bacteremia MLAB 2434 –Microbiology Keri Brophy-Martinez
Definitions • Pseudobacteremia • False bacteremia • Contamination of a blood culture during or after collection
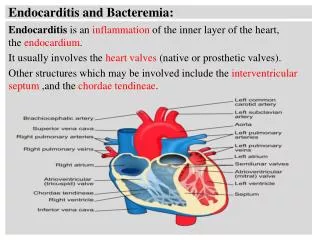
Definitions • Bacteremia – presence of bacteria in blood stream • Some conditions have a period of bacteremia as part of the disease process (ex. Meningitis, endocarditis) • Usually occurs due to a disruption of skin or mucosal barriers to bacterial invasion
Classifications of Bacteremia • Classified by Site of Origin • Classified by Causative Agent • Classified by Place of Acquisition • Classified by Duration
Classification by Site of Origin • Primary Bacteremia • Blood stream or endovascular bacterial invasion with no preceding or simultaneous site of infection with the same microorganism • Secondary Bacteremia • Isolation of a microorganism from blood as well as other site(s) • Fever of Unknown Origin (FUO) • Source unknown
Classification by Causative Agent • Gram positive bacteremia • Gram negative bacteremia • Anaerobic bacteremia • Polymicrobial bacteremia
Classification by Place of Acquisition • Community-acquired • Health-care acquired/Nosocomial • Defined as occurring 72 hours post admission
Classification by Duration • Transient • Comes and goes • Usually occurs after a procedural manipulation (ex. Dental procedures) • Intermittent • Can occur from abscesses at some body site that is “seeding” the blood • Continuous Bacteremia • Organisms from an intravascular source that are consistently present in bloodstream
Sepsis & Septicemia • Presence of active bacteria • Results from continuous bacteremia • Clinical signs and symptoms of bacterial invasion and toxin production • Apply the SIRS criteria • Systemic response to bacterial infection
Bacteremia Complications • Septic shock • Results from body’s reactions to bacterial bi-products • Endotoxins: lipopolysaccharide • Exotoxins • Disrupts many body functions • Hemodynamic changes, decreased tissue perfusion and compromised organ & tissue function • Mortality 40% to 50%
Bacteremia/Septicemia Risk Factors • Immunocompromised patients • Due to decrease in circulating neutrophils • Increased use of invasive procedures & indwelling devices • Disrupts normal flora • Age of patient • Young: defect in humoral immunity • Old: Decreased immune competency • Administration of drug therapy • Broad spectrum antibiotics decrease normal flora • Increase in antimicrobial resistance
Sources of Bacteremia • Pericarditis and Peritonitis • Pneumonias • Pressure sores • Prosthetic medical devices • Total hip replacement • Skeletal system • Skin and soft tissue • Urinary Tract Infections
Clinical Signs and Symptoms • Abrupt onset of chills, fever, or hypothermia and hypotension • Prostration (exhaustion/weakness) and diaphoresis (perspiration) • Tachypnea (rapid breathing) is an early sign of bacteremia • Delirium, stupor, agitation • Nausea, vomiting
Clinical Signs and Symptoms (cont’d) • Laboratory Values in Bacteremia • Thrombocytopenia • Leukocytosis or leukopenia • Acidosis • Abnormal liver functions • Coagulopathy • DIC • Elevations in CRP, haptoglobin, fibrinogen, ESR, procalcitonin
Specimen Collection • Positive blood cultures • Critical value • Physician correlates finding to clinical picture to verify septicemia • Best Practice • Collect specimen immediately PRIOR to rise in temperature • Collect PRIOR to antibiotic therapy
Specimen Collection • Aseptic collection procedure is critical • Cleansing agents • Tincture of iodine (1-2%) • Leave on skin for 30 seconds • Povidine-iodine (10%) • Leave on skin 1.5 to 2 minutes • Chlorhexidine/ChloraPrep • Leave on skin for 30 seconds • 2% chlorhexidine gluconate + 70% isopropyl alcohol • Cleansing Technique • In concentric fashion, from inside to out • After cleaning, wait 1.5-2 minutes • Acceptable Contamination Rate • 1-3%
Collection sites • Preferred • Peripheral venous • Arterial sites • Less common • Central venous catheters • Arterial lines
Blood Collection Devices • Traditional set • Aerobic bottle • Selects for aerobic & facultative anaerobes • Anaerobic bottle • Selects for obligate anaerobes • ARD bottle (Antibiotic Removal Device) • Used when patient is on antibiotics prior to blood collection • SPS= Sodium polyanetholsulfonate
Blood Collection Devices • Anticoagulants • SPS= Sodium polyanetholsulfonate • Function/Purpose • Anticoagulant • Neutralizes human serum • Prevents phagocytosis • Inactivates certain antimicrobial agents • SAS(sodium amylosulfate) • Similar to SPS, but less effective in neutralizing serum
Specimen Collection:Blood Volume • Ideal ratio of blood: broth • 1:5 to 1:10 • Dilution aids in preventing the bactericidal effect of WBCs & complement • Volume Recommendations by Age • Younger than 10 years- 1 mL of blood for every year of life • Over 10 years- 20 mL • Short draw? • Inoculate anaerobic bottle first
Specimen Collection:Frequency of Collection • Depends if bacteremia is transient, intermediate or continuous • General guidelines • Usually x2 from different body sites, when patient is spiking a fever • Endocarditis • 3 sets from 3 different sites within 1-2 hours of clinical presentation • Fever of Unknown Origin (FUO) • Initially 2 sets; 24-36 hours later, obtain 2 more
Specimen Collection:Frequency of Collection • If a catheter-related bloodstream infection is suspected: • One set drawn peripherally • One set drawn via catheter
Blood Culture Methods • Conventional Broth Systems • Aerobic broth contains soybean casein digest broth, tryptic or trypticase soy broth, Brucella agar or Columbia broth base • Anaerobic broth is usually the same as aerobic with addition of 0.5% cysteine in an aerobic environment • Must be subcultured and gram stained manually, at 12, 24 and 48 hours • Method not recommended due to risk of needlestick and contamination; not cost effective
Blood Culture Methods (cont’d) • Biphasic Broth-Slide System • Agar “paddles” attached to top of bottle; includes CA, MAC, malt extract agars • Incubate at 35 OC for 7 days • Allows for blind subcultures • Closed system
Blood Culture Methods (cont’d) • Lysis-Centrifugation Blood Culture Systems (Isolator) • Used in the recovery of Fungus and AFB • The Isolator is a special tube that contains saponin, a chemical that lyses cells and other anticoagulants • Approximately 7.5-10 ml of blood is placed in the tube, then centrifuged to concentrate microorganisms; sediment is subcultured to fungal and/or mycobacterial media
Blood Culture Methods (cont’d) • Automatic Blood Culture Systems • BacTec 9000 Series • Fluorescent light is used to detect changes in CO2 levels
Automatic Blood Culture Systems (con’t) • ESP( Extra Sensing Power) • Now VersaTREK • Measures consumption/production of gases; such as CO2 H2, N2 and O2 in the headspace of each bottle • Detects a change in pressure
Automatic Blood Culture Systems (con’t) • BacT-Alert • Carbon dioxide production results in a pH change • pH change results in color change detected by system as “positive”
Blood Culture Workup • Incubation times • Routine aerobic/anaerobic • 5-7 days • Endocarditis • 2 weeks • Brucellosis/Fungemia/HACEK • 21-28 days • Reporting results • Initial report is sent out at 24 hours • Final report is sent out at 5-7 days for all no growth specimens
Blood Culture Workup • Positive Cultures • Gram stain the bottle to determine the morphology of the organism present • Call the results of the gram stain to the physician or nurse, including how many sets etc., so that antibiotic therapy can be initiated • Subculture to appropriate media • Identify organism and perform sensitivity testing
Blood Cultures: Pathogens • Staphylococcus aureus • Streptococcus pneumoniae • Haemophilus influenza • Pseudomonas species • Neisseria species • Coagulase negative Staphylococcus species (immunocompromised) • Group B Streptococcus (infants) • Alpha hemolytic Streptococcus viridans group • Gram negative rods • Yeasts and molds • Anaerobes
Blood Cultures: Contaminants • Coagulase negative Staphylococcus • Propionibacterium acnes • Alpha hemolytic Streptococcus viridans group • Bacillus species • Diphtheroids • Growth of multiple organism
Treatment & Prevention • Treatment • Empirical treatment, initially, with broad spectrum antibiotic • Antisepsis therapy; physiological support, anticoagulation agents, glucocorticoids • Adjunctive measures; draining fluids, removing catheters • Prevention • Vaccines; S. pneumo, influenza, varicella
References • Broyles, M. (2013, June). A Closer Look at Sepsis. ADVANCE for Medical Laboratory Professionals, 25(5), 12-13. • http://www.achats-publics.fr/Fournisseurs/BIOMERIEUX.htm http://www.bd.com/ds/productCenter/212536.asp • http://www.bd.com/ds/productCenter/445718.asp • http://www.temple.edu/medicine/microbiology_lab.htm • Kiser, K. M., Payne, W. C., & Taff, T. A. (2011). Clinical Laboratory Microbiology: A Practical Approach . Upper Saddle River, NJ: Pearson Education. • Mahon, C. R., Lehman, D. C., & Manuselis, G. (2011). Textbook of Diagnostic Microbiology (4th ed.). Maryland Heights, MO: Saunders.