Download
1 / 12
120 likes | 352 Views
Acute ET in a 42 yo male with recent diarrhoea. OMC Fumtiaka Nonaka. 17/10/2011 ED (2wk from onset). 42yo Male c/o binocular diplopia (mainly horizontal, with vertical and torsional component) difficulty in focusing, pain behind the eyes for 2/52

E N D
Acute ET in a 42 yo male with recent diarrhoea OMC Fumtiaka Nonaka
17/10/2011 ED (2wk from onset) • 42yo Male • c/o binocular diplopia (mainly horizontal, with vertical and torsional component) • difficulty in focusing, pain behind the eyes for 2/52 • 3-4/52 ago had acute gastroenteritis, pins and needles, unbalanced • denies: ataxia, inco-ordination, other motor/sensory symptoms • POH: red-green color blindness • PMH: nil, no head trauma
On Examination in ED • VA: R 6/5-3, L 6/9+3 • Ishihara 2/15, R+L • no RAPD • CT: Alternating ET (PCT: not performed) • EOM: LLR-, RIO+, LSR-, end point nystagmus, normal saccades, pain on looking up, no INO • Bloods: FBE, U+E normal, CRP<1, RF –ve, TSH WNL, ANA detected(titre 1:80, <1:80 = negative) • MRI brain (25/10/11): normal, no evidence for intracranial demyelination
What’s next? Anti-ganglioside antibodies
04/11/11 OMC (5wk from onset) • VA: R 6/5 L 6/6 • HVF: W.N.L. • EOM: RLR-, LLR- (see Hess) • PCT: Near 35ΔET’ LH’6Δ Distance 50ΔET LH6Δ • Bloods: • GQ1b IgG Ab +ve • MAG IgM IFA –ve • GM1 IgG Ab –ve, GM1 IgM Ab –ve • AChR Ab –ve
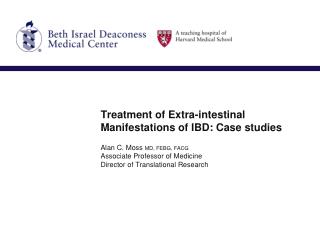
18/11/11 OMC (7wk) • Much better, SV in am, gradually develops diplopia as day progresses • EOM RLR-, LLR- (see Hess) • PCT: Near 14ΔET’ LH’3Δ Distance 25ΔET LH3Δ • Saccades fast and accurate, no fatigue 02/12/11 OMC (9wk) • S: still diplopia to sides, after midday • PCT: Near 6ΔET’ LH’3Δ • Distance 6ΔET LH2Δ (see Hess)
04/11/11 (5wk) 18/11/11 (7wk) Distance 50ΔET LH6Δ Distance 25ΔET LH3Δ 02/12/11 (9wk) Distance 6ΔET LH2Δ
Miller-Fisher syndrome ´ • a variant of Guillain-Barre syndrome • a triad of ophthalmoplegia, ataxia, and areflexia • full triad of MFS is not always present • anti-GQ1b ganglioside antibodies +ve in 90% of MFS • Campylobacter jejuni, cytomegalovirus, Epstein-Barr virus, and Streptococcus pyogenes have been reported as antecedent infectious agents in MFS. (J Neurol Sci 1998;160:64–6) • good recovery with or without treatment Charles Miller Fisher MD 1913 - 2011
Anti-GQ1b antibody • Acute conditions Miller-Fisher Syndrome Acute ophthalmoparesis (ophthalmoplegia without ataxia) • Chronic conditions Otherwise unexplained ophthalmoplegia Anti-Gq1b * Abundant staining anti-GQ1b Abs: NMJs of human EOMs > limb muscles *NMJ = Neuromuscular junction NMJs of EOMs may be easily targeted by anti-GQ1b Abs Absence of a blood-nerve barrier High capillary supply Immunolocalization of GQ1b and Related Gangliosides in Human Extraocular Neuromuscular Junctions and Muscle Spindles. F. Pedrosa-Domellof et al, IOVS 2009;50:3226 –3232
Anti-ganglioside antibodies& diplopia • “ANTI GM1 ANTIBODIES – THE CAUSE OF OTHERWISE UNEXPLAINED • OPHTHALMOLPLEGIAS?” L Kowal et al, 2003 • Four patients with otherwise unexplained ophthalmoplegia • No other neurological problems • Elevated levels of IgM GM1 Ab • Normal anti-GQ1b Ab • Anti-GQ1b IgG antibody syndrome: clinical and immunological range. • K Hirata, et al, J Neurol Neurosurg Psychiatry 2001;70:50–55 • 194 patients with anti-GQ1b IgG • 94% had antecedent illnesses • 84% upper respiratory tract infection • 10% diarrhoea • As initial symptoms • 67% diplopia • 29% gait disturbance
The case described might be labelled “ophthalmoparesis due to presumed microvascular causes” or “presumed breakdown of latent squint” as no other explainable causes have been found. • Measurement of anti-ganglioside antibodies should be considered in cases of otherwise unexplained ophthalmoplegia.