Download
1 / 1
10 likes | 123 Views
Colorectal cancer screening with the addition of flexible sigmoidoscopy to guaiac-based fecal occult blood testing: a population-based controlled trial. Wintzenheim. Bernard DENIS, Isabelle GENDRE,,Jean Christophe PFEIFFER, Anne Marie WEISS, Frédéric VAGNE, André PETER, Philippe PERRIN.

E N D
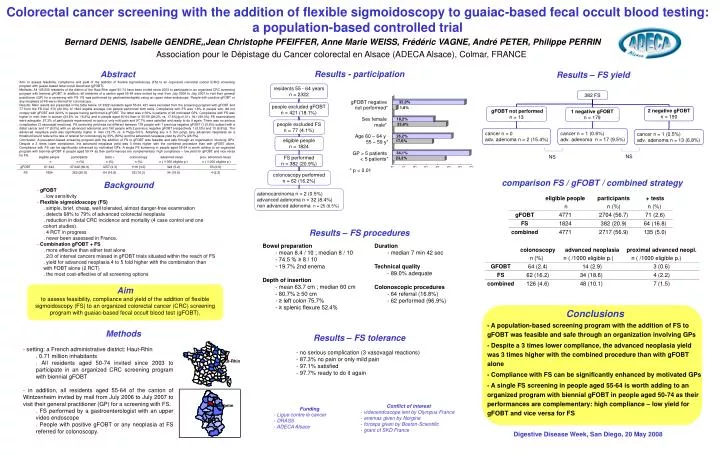
Colorectal cancer screening with the addition of flexible sigmoidoscopy to guaiac-based fecal occult blood testing: a population-based controlled trial Wintzenheim Bernard DENIS, Isabelle GENDRE,,Jean Christophe PFEIFFER, Anne Marie WEISS, Frédéric VAGNE, André PETER, Philippe PERRIN Association pour le Dépistage du Cancer colorectal en Alsace (ADECA Alsace), Colmar, FRANCE Results - participation Abstract Results – FS yield Aim: to assess feasibility, compliance and yield of the addition of flexible sigmoidoscopy (FS) to an organized colorectal cancer (CRC) screening program with guaiac-based fecal occult blood test (gFOBT). Methods: All 185,000 residents of the district of the Haut-Rhin aged 50-74 have been invited since 2003 to participate in an organized CRC screening program with biennial gFOBT. In addition, all residents of a canton aged 55-64 were invited by mail from July 2006 to July 2007 to visit their general practitioner (GP) for a screening with FS. FS was performed by gastroenterologists using an upper video-endoscope. People with positive gFOBT or any neoplasia at FS were referred for colonoscopy. Results: Main results are presented in the table below. Of 2322 residents aged 55-64, 421 were excluded from the screening program with gFOBT and 77 from the FS trial. 370 (20.3%) of 1824 eligible average risk people performed both tests. Compliance with FS was 1.8% in people who did not comply with gFOBT and 32.0% in people having performed a gFOBT. The latter was ≥ 50% in patients of 26 motivated GPs. Compliance with FS was higher in men than in women (23.8% vs. 18.2%) and in people aged 60-64 than in 55-59 (26.2% vs. 17.6%)(p<0.01). 341 (89.3%) FS examinations were adequate. 87.3% of participants experienced no pain or only mild pain and 97.7% were satisfied and ready to do it again. There was no serious complication (3 vasovagal reactions). FS screening yield was not different between 179 people with 1 previous negative gFOBT (1 (0.6%) subject with a distal cancer and 17 (9.5%) with an advanced adenoma) and 190 people with 2 previous negative gFOBT (respectively 1 (0.5%) and 13 (6.8%)). The advanced neoplasia yield was significantly higher in men (12.7% vs. 4.1%)(p<0.01). Adopting any ≥ 5 mm polyp (any advanced neoplasia) as a threshold would reduce the rate of referral for colonoscopy by 35% (50%) and the advanced neoplasia yield by 23.5% (26.5%). Conclusion: A population-based screening program with the addition of FS to gFOBT was feasible and safe through an organisation involving GPs. Despite a 3 times lower compliance, the advanced neoplasia yield was 3 times higher with the combined procedure than with gFOBT alone. Compliance with FS can be significantly enhanced by motivated GPs. A single FS screening in people aged 55-64 is worth adding to an organized program with biennial gFOBT in people aged 50-74 as their performances are complementary: high compliance – low yield for gFOBT and vice versa for FS. gFOBT negative not performed* Sex female male* Age 60 – 64 y 55 – 59 y* GP > 5 patients < 5 patients* * p < 0.01 NS NS comparison FS / gFOBT / combined strategy Background • gFOBT • . low sensitivity • Flexible sigmoidoscopy (FS) • . simple, brief, cheap, well tolerated, almost danger-free examination • . detects 68% to 79% of advanced colorectal neoplasia • . reduction in distal CRC incidence and mortality (4 case control and one cohort studies) • . 4 RCT in progress • . never been assessed in France. • Combination gFOBT + FS • . more effective than either test alone • . 2/3 of interval cancers missed in gFOBT trials situated within the reach of FS • . yield for advanced neoplasia 4 to 5 fold higher with the combination than with FOBT alone (2 RCT) • . the most cost-effective of all screening options Results – FS procedures • Bowel preparation • - mean 8.4 / 10 ; median 8 / 10 • - 74.5 % ≥ 8 / 10 • - 19.7% 2nd enema • Depth of insertion • - mean 63.7 cm ; median 60 cm • - 80.7% ≥ 50 cm • - ≥ left colon 75.7% • - ≥ splenic flexure 52.4% • Duration • - median 7 min 42 sec • Technical quality • - 89.0% adequate • Colonoscopic procedures • - 64 referral (16.8%) • - 62 performed (96.9%) Aim to assess feasibility, compliance and yield of the addition of flexible sigmoidoscopy (FS) to an organized colorectal cancer (CRC) screening program with guaiac-based fecal occult blood test (gFOBT). Conclusions - A population-based screening program with the addition of FS to gFOBT was feasible and safe through an organization involving GPs - Despite a 3 times lower compliance, the advanced neoplasia yield was 3 times higher with the combined procedure than with gFOBT alone - Compliance with FS can be significantly enhanced by motivated GPs - A single FS screening in people aged 55-64 is worth adding to an organized program with biennial gFOBT in people aged 50-74 as their performances are complementary: high compliance – low yield for gFOBT and vice versa for FS Methods Results – FS tolerance • setting: a French administrative district: Haut-Rhin • . 0.71 million inhabitants • . All residents aged 50-74 invited since 2003 to participate in an organized CRC screening program with biennial gFOBT • - in addition, all residents aged 55-64 of the canton of Wintzenheim invited by mail from July 2006 to July 2007 to visit their general practitioner (GP) for a screening with FS. • . FS performed by a gastroenterologist with an upper video endoscope • . People with positive gFOBT or any neoplasia at FS referred for colonoscopy. • no serious complication (3 vasovagal reactions) • 87.3% no pain or only mild pain • 97.1% satisfied • 97.7% ready to do it again Haut-Rhin • Conflict of interest • videoendoscope lent by Olympus France • enemas given by Norgine • forceps given by Boston-Scientific • grant of SKD France • Funding • Ligue contre le cancer • DRASS • ADECA Alsace Digestive Disease Week, San Diego, 20 May 2008