Download
1 / 1

E N D
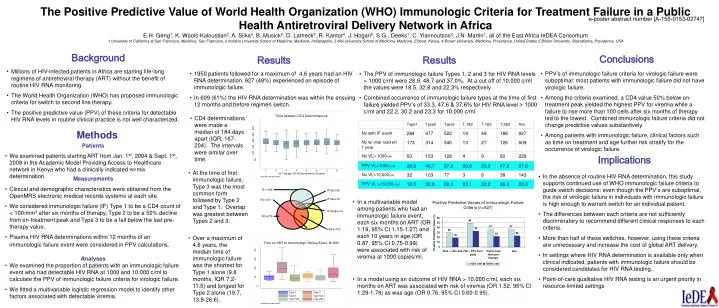
e-poster abstract number [A-155-0153-02747] The Positive Predictive Value of World Health Organization (WHO) Immunologic Criteria for Treatment Failure in a Public Health Antiretroviral Delivery Network in AfricaE.H. Geng1, K. Wools-Kaloustian2, A. Siika3, B. Musick2, D. Lameck3, R. Kantor4, J. Hogan5, S.G., Deeks1, C. Yiannoutsos2, J.N. Martin1, all of the East Africa IeDEA Consortium1 University of California at San Francisco, Medicine, San Francisco, 2 Indiana University School of Medicine, Medicine, Indianapolis, 3 Moi University School of Medicine, Medicine, Eldoret, Kenya, 4 Brown University, Medicine, Providence, United States,5 Brown University, Biostatistics, Providence, USA Conclusions Background Results Results • Millions of HIV-infected patients in Africa are starting life-long regimens of antiretroviral therapy (ART) without the benefit of routine HIV RNA monitoring. • The World Health Organization (WHO) has proposed immunologic criteria for switch to second line therapy. • The positive predictive value (PPV) of these criteria for detectable HIV RNA levels in routine clinical practice is not well characterized. • 1950 patients followed for a maximum of 4.6 years had an HIV RNA determination. 927 (48%) experienced an episode of immunologic failure. • In 609 (61%) the HIV RNA determination was within the ensuing 12 months and before regimen switch. • PPV’s of immunologic failure criteria for virologic failure were suboptimal: most patients with immunologic failure did not have virologic failure. • Among the criteria examined, a CD4 value 50% below on-treatment peak yielded the highest PPV for viremia while a failure to rise more than 100 cells after six months of therapy led to the lowest. Combined immunologic failure criteria did not change predictive values substantively. • Among patients with immunologic failure, clinical factors such as time on treatment and age further risk stratify for the occurrence of virologic failure. • The PPV of immunologic failure Types 1, 2 and 3 for HIV RNA levels > 1000 c/ml were 28.9, 48.7 and 37.0%. At a cut off of 10,000 c/ml the values were 18.5, 32.8 and 22.3% respectively. • Combined occurrence of immunologic failure types at the time of first failure yielded PPV’s of 33.3, 47.6 & 37.6% for HIV RNA level > 1000 c/ml and 22.2, 30.2 and 23.3 for 10,000 c/ml. • CD4 determinations were made a median of 184 days apart (IQR, 167-204). The intervals were similar over time. Methods • Patients • We examined patients starting ART from Jan. 1st, 2004 & Sept. 1st, 2008 in the Academic Model Providing Access to Healthcare network in Kenya who had a clinically indicated HIV RNAdetermination. Implications • At the time of first immunologic failure, Type 3 was the most common form followed by Type 2 and Type 1. Overlap was greatest between Types 2 and 3. • In the absence of routine HIV RNA determination, this study supports continued use of WHO immunologic failure criteria to guide switch decisions: even though the PPV’s are suboptimal, the risk of virologic failure in individuals with immunologic failure is high enough to warrant switch for an individual patient. • The differences between each criteria are not sufficiently discriminatory to recommend different clinical responses to each criteria. • More than half of these switches, however, using these criteria are unnecessary and increase the cost of global ART delivery. • In settings where HIV RNA determination is available only when clinical indicated, patients with immunologic failure should be considered candidates for HIV RNA testing. • Point-of-care qualitative HIV RNA testing is an urgent priority in resource-limited settings • Measurements • Clinical and demographic characteristics were obtained from the OpenMRS electronic medical records systems at each site. • We considered immunologic failure (IF) Type 1 to be a CD4 count of < 100/mm3 after six months of therapy, Type 2 to be a 50% decline from on-treatment peak and Type 3 to be a fall below the last pre-therapy value. • Plasma HIV RNA determinations within 12 months of an immunologicfailure event were considered in PPV calculations. • In a multivariable model among patients who had an immunologic failure event, each six months on ART (OR 1.19, 95% CI 1.15-1.27) and each 10 years in age (OR 0.87, 95% CI 0.75-0.99) were associated with risk of viremia at 1000 copies/ml. • Over a maximum of 4.6 years, the median time of immunologic failure was the shortest for Type 1 alone (9.8 months, IQR 7.2-11.5) and longest for Type 2 alone (19.7, 13.8-26.6). • Analyses • We examined the proportion of patients with an immunologic failure event who had detectable HIV RNA at 1000 and 10,000 c/ml to calculate the PPV of immunologic failure criteria for virologic failure. • We fitted a multivariable logistic regression model to identify other factors associated with detectable viremia. • In a model using an outcome of HIV RNA > 10,000 c/ml, each six months on ART was associated with risk of viremia (OR 1.52, 95% CI 1.29-1.78) as was age (OR 0.76, 95% CI 0.60-0.95).