Download
1 / 70
720 likes | 1.07k Views
Interventions for Clients with Breast Disorders. Anatomy and Physiology. Paired mammary glands within the superficial fascia of the chest wall Female breast extends vertically from the 2nd or 3rd rib to 6th or 7th Laterally from sternal margin to midaxillary line.

E N D
Anatomy and Physiology Paired mammary glands within the superficial fascia of the chest wall Female breast extends vertically from the 2nd or 3rd rib to 6th or 7th Laterally from sternal margin to midaxillary line. Breast is usually divided into 4 quadrants
4 quadrants to describe clinical findings The upper outer quadrent is the site of most breast tumors Topography of Breast
Anatomy and Physiology: Female Breast • Three types of tissue: glandular, subcutaneous and retromammary fat, and fibrous • Glandular: 20 lobes per breast which radiates around the nipple in spoke like pattern. Most glandular tissue lies in the upper outer quadrant. From here the breast extends into the axilla forming the Tail of Spence.
SCREENING RECOMMENDATIONS SCREENING MAMMOGRAM (Baseline) at age 40, and annually after age 40-50. (Best 1 week after menstrual period) BREAST SELF EXAM monthly, begin @ age 20 CLINICAL BREAST EXAM yearly after age 40
CLINICAL BREAST EXAM yearly after age 40 • BARRIERS: • fear of pain, radiation, results • accessibility, cost • modesty • knowledge deficit
CANCER SCREENING: HIGH RISK • Screening:BSE monthly, age 20 • CBE q6-12 mo., ages 25-35 • Mammography annually, ages 25-35 years of age Options: • Decrease risk factors? • Prophylactic mastectomy • Chemoprevention • (Tamoxifen & other newer drugs)
GOAL: Early detection IN PREPARATION FOR TEACHING: Assess: knowledge base , motivation fears and concerns family history risk factors TEACHING: Use show and tell; use finger pads EXAM: monthly, day 5-7 of menstrual cycle; after menopause same day each month Use in conjunction with mammography & CBE BREAST SELF EXAM
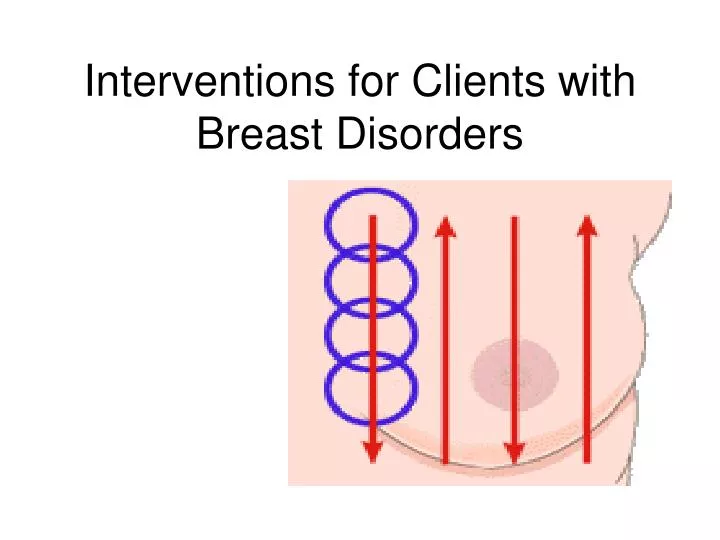
Begin by looking at your breasts in the mirror with your shoulders straight and your arms on your hips. Here's what you should look for: Breasts that are their usual size, shape, and color. Breasts that are evenly shaped without visible distortion or swelling. If you see any of the following changes, bring them to your doctor's attention: Dimpling, puckering, or bulging of the skin. A nipple that has changed position or become inverted (pushed inward instead of sticking out). Redness, soreness, rash, or swelling. Breast Self Exam - Step 1
Raise your arms and look for the same changes. While you're at the mirror, gently squeeze each nipple between your finger and thumb and check for nipple discharge (this could be a milky or yellow fluid or blood). Breast Self Exam - Step 2 and 3
Feel your breasts while lying down, using your right hand to feel your left breast and then your left hand to feel your right breast. Use a firm, smooth touch with the first few fingers of your hand, keeping the fingers flat and together. Cover the entire breast from top to bottom, side to side—from your collarbone to the top of your abdomen, and from your armpit to your cleavage. Breast Self Exam - Step 4
Finally, feel your breasts while you are standing or sitting. Many women find that the easiest way to feel their breasts is when their skin is wet and slippery, so they like to do this step in the shower. Cover your entire breast, using the same hand movements described in Step 4. Breast Self Exam - Step 5
CLINICAL BREAST EXAM • HISTORY: (Subjective data) • Onset of problem? • What symptoms? • Pain associated with symptoms? • Self breast examination practices? Mammograms? • Reproductive history? • Tobacco & alcohol use? • Medical & surgical history? • Socio-economic information?
Symmetry Size Contour Skin color, venous pattern, changes (edema or pitting) Nipple changes Lesions Discharge- type, color Mass Axillary area Area over clavicle BREAST ASSESSMENT: INSPECTION & PALPATION
Equipment Needed • None • The patient must be properly gowned for this examination. All upper body clothing should be removed.
General Considerations • The patient must be properly gowned for this examination. All upper body clothing should be removed. • Breast tissue changes with age, pregnancy, and menstrual status. • The procedure described here can also be used for self-examination using a mirror for inspection.
Inspection • Give a brief overview of examination to patient. [1] • Have the patient sit at end of exam table. • Ask the patient to remove gown to her waist, assist only if needed. • Have the patient relax arms to her side. • Examine visually for following: • Approximate symmetry • Dimpling or retraction of skin • Swelling or discoloration • Orange peel effect on skin • Position of nipple • Observe the movement of breast tissue during the following maneuvers: • Shrug shoulders with hands on hips • Slowly raise arms above head • Lean forward with hands on knees (large breasts only) • Have the patient replace the gown. • Reassure the patient, if the exam is normal so far, say so.
Palpation • Have the patient lie supine on the exam table. • Ask the patient to remove the gown from one breast and place her hand behind her head on that side. • Begin to palpate at junction of clavicle and sternum using the pads of the index, middle, and ring fingers. If open sores or discharge are visible, wear gloves. • Press breast tissue against the chest wall in small circular motions. Use very light pressure to assess superficial layer, moderate pressure for middle layer and firm pressure for deep layers. • Palpate the breast in overlapping vertical strips. Continue until you have covered the entire breast including the axillary "tail." [2] • Palpate around the areola and the depression under the nipple. Press the nipple gently between thumb and index finger and make note of any discharge. • Lower the patient's arm and palpate for axillary lymph nodes. • Have the patient replace the gown and repeat on the other side. • Reassure the patient, discuss the results of the exam.
Fibroadenoma – benign, glandular and fibrous, small, rubbery, nontender
BENIGN BREAST DISORDERSFIBROADENOMA • Most common cause of breast masses, especially in teens & young women (to early 30’s) • Often upper, outer quadrant • Solid, slowly enlarging, benign mass, unattached to surrounding breast tissue • Usually round, firm, easily movable, nontender, clearly distinct from surrounding tissue • Enlarges slowly
FIBROCYSTIC BREAST DISEASE Most common in adult women, ages 20-30 Ducts dilate & cysts form, more diffuse May occur in stages: Stage 1: premenstrual sx, bilateral, 20’s Stage 2: sx +, bilateral, nodular, 30’s Stage 3: cystic, smooth, painful or tender, 35-55
FIBROCYSTIC BREAST DISEASE • Treatment (usually symptomatic) may include: • Hormones (oral contraceptives, estrogen, progestin, Danazol) • Vitamins C, E, B complex • Diuretic agents • NaCl, avoid caffeine • Anti-inflammatory meds (Ibuprofen) as needed • Wear supportive bra • Heating pad, ice
DUCTAL ECTASIA • Dilation & thickening of ducts in subareolar area • Occurs usually in women nearing menopause • Masses due to inflammatory response, may feel tender, hard, irregular (may be difficult to distinguish from malignancy) • Redness, edema over mass site • Greenish-brown nipple discharge • Enlarged axillary nodes
Ductal ecstasia – benign, inflamed and dilated, subareolar duct, nipple discharge green/black and sticky, can become abscess
INTRADUCTAL PAPILLOMA • Occurs usually in women nearing menopause • Rarely palpable mass • Serosanguineous nipple discharge (usually microscopic exam of discharge) • Surgical excision if indicated
OTHER BENIGN BREAST DISORDERSLarge breasts • Disproportionate to rest of body • Difficult, expensive to find clothes to fit • Can cause backaches • Can cause fungal infections under breasts • Can be treated by REDUCTION • MAMMOPLASTY
GYNECOMASTIA ( breast size in male) • Can be secondary to other diseases such as lung Ca • 90% bilateral • May be due to: • Aging • Estrogen excess (malnutrition, liver disease, hyperthyroidism) • Androgen deficiency • Obesity • Drugs • Chronic renal failure
BREAST CANCER • Most diagnosed invasive cancer in females • Second leading cause of breast masses & cancer deaths overall • 80% diagnosed in women over age 50 • Early detection & treatment key to survival • Localized with no regional spread: cure 75%-90% • 5 and 10 year survival rates drop with axillary lymph node involvement • Incidence lower in African-American & Hispanic women, but death rates higher (highest death rate is Hawaiian)
BREAST CANCER: ETIOLOGY/ RISK FACTORS • 70% women diagnosed with breast cancer have no identifiable risk factors other than age & gender • Age: > 45, as age , risk • History: client’s & family’s • 3X in females with affected 1st degree relative (but 90% have no affected relatives) • in women with multiple affected 1st degree relatives, or if relative has Ca bilaterally or diagnosed at early age
Invasive Ca – ducts or lobules, irregular, poorly delineated
Non invasive Ca – ductal in situ or lobular in situ, abnormal mammogram
risk in early menarche (before 12) & late menopause • in nulliparity or 1st pregnancy after age 30 • in exposure to ionizing radiation (esp. before age 20) • with hx of previous breast Ca, & risk for recurrence if diagnosed at earlier age or with hx of ovarian Ca • with age
QUESTIONABLE RISK FACTORS • Diet: high in animal fats, low in fiber • Obesity • Oral contraceptives • Alcohol/ Tobacco • Hormone replacement rx > 5 years
BREAST CANCER: PREVENTION IN HIGH RISK WOMEN • TAMOXIFEN: results of Breast Cancer Prevention Trial in women high risk for breast Ca-> those receiving had Ca by 45% • EVISTA: lower incidence of Breast Ca • ARIMIDEX: new Ca prevention drug being studied • PROPHYLACTIC MASTECTOMY: • often with immediate reconstruction
BREAST CANCERINFILTRATING DUCTAL CARCINOMA • Most common, 80% of all breast Ca’s • Hardness on palpation, may be 5-9 years before mass is palpable • May be NONINVASIVE (remain in duct) or INVASIVE (penetrate surrounding tissue causing irregular mass) • As grows, fibrosis develops, causes shortening of Cooper’s ligaments, causes skin dimpling (more advanced disease) • Often metastasizes to axillary nodes
COMPLICATIONS OF BREAST CANCER • Tumor invades lymphatic channels • Blocks skin drainage causing skin edema & “orange peel” appearance, may -> skin breakdown • Metastasis occurs from seeding of CA cells into blood and lymph systems • Most common metastatic sites are *bone, lungs, brain, and liver
BREAST CANCER IN MEN • 1% of all cases of breast cancer • Average onset 60 years of age • Risk factors: hx of mumps orchitis, Klinefelter’s syndrome • Symptoms can include: • Hard, nonpainful, subareolar lesion • Nipple erosion, retraction, or discharge (75% have Ca) • Treatment: modified radical mastectomy with radiation • v 5 year survival rates are only 58% in Stage 1
ASSESSMENT: BREAST CANCERHISTORY: • Risk Factors • Mass • When & by whom discovered When sought care • Health maintenance practices: • BSE, Mammograms, Diet, Alcohol use, • Medications including hormone supplements
BREAST CANCER: PHYSICAL ASSESSMENTMASS • Location – usually upper, outer quadrant of breast • Size • Shape • Hard consistency, with irregular borders • Fixed, not movable • Nipple, Skin Changes (orange peel appearance, ulceration, shortening of Cooper’s ligaments with dimpling) • Lymph nodes • Usually nontender, painfree unless in later stages
PSYCHOSOCIAL ASSESSMENT • Fear of cancer & prognosis • Previous experiences with cancer • Knowledge, education level • Threats to body image • Threats to sexuality and intimate relationships • Support systems • Need for other resources or counseling
BREAST ASSESSMENT • SBE • CBE • Mammography, Galactography • Ultrasound • MRI
DIAGNOSTIC ASSESSMENTLABORATORY: • Pathology reports • Study of cancer markers • Liver enzymes • Serum calcium • Alkaline phosphatase
RADIOGRAPHIC • Mammography • Chest X ray • Bone Scan • Brain Scan • Liver Scan • CT- Chest and abdomen
DIAGNOSTIC ASSESSMENT • Ultrasonography- differentiates fluid filled from solid masses • Breast biopsy with pathology report • Estrogen and progesterone receptors (women with ER + tumors have longer survival rate) • Tumor cell differentiation (women with well differentiated tumors have longer survival) • Pathology exam of lymph nodes
BREAST BIOPSY INDICATED: • If needle aspirated fluid is bloody • No fluid is aspirated from lesion • Suspicious mammogram • Mass still present after aspiration • Cytological study shows malignant cells
BREAST BIOPSY:NURSING CARE Assess anxiety & fear (80% are negative) Education • Prior to biopsy, avoid agents interfering with blood clotting • NPO • Care of biopsy site • Avoid strenuous exercises for 1 week • Pain management • Supportive bra for 3-7 days Post test: Monitor: • Effects of anesthesia • Toleration of fluids, food, ambulation
BREAST CANCER STAGING • STAGE 1 • Tumor smaller than 2cm & no lymph node involvement • STAGE 2 • Tumor 2-5 cm with 0-1 + lymph nodes • STAGE 3 (no metastasis evident) • Tumor larger than 5cm, no + lymph nodes or • Smaller than 2 cm, with + lymph nodes, or • 2-5 cm with + nodes • STAGE 4 • Tumor of any size, + or – lymph nodes, with distant metastasis evident