Download
1 / 64
640 likes | 847 Views
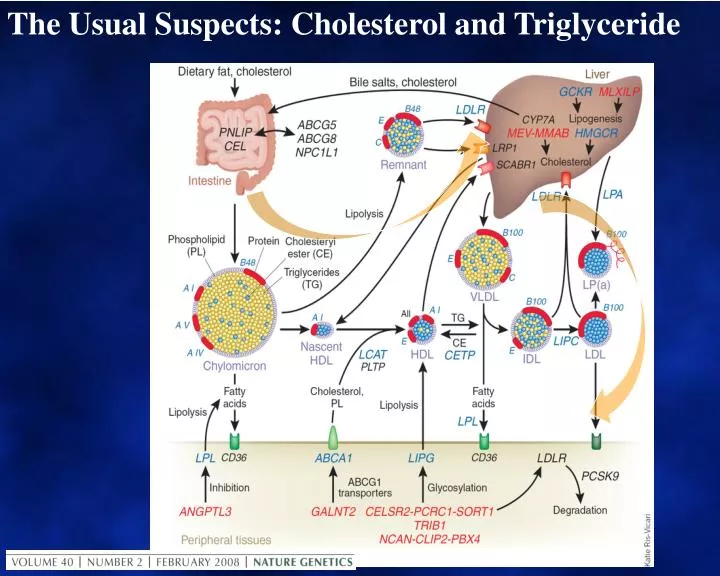
The Usual Suspects: Cholesterol and Triglyceride. Lipid Structure. Cholesterol: Membranes Bile Acids Steroid Hormones Protein modification. HO. Fatty Acids: Fuel, Prostanoids. Triglycerides: FA for Fuel, Prostanoids Protein modification. COOH. COO. COOH. COO. COOH.

E N D
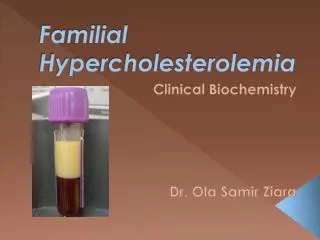
Lipid Structure Cholesterol: Membranes Bile Acids Steroid Hormones Protein modification HO Fatty Acids: Fuel, Prostanoids Triglycerides: FA for Fuel, Prostanoids Protein modification COOH COO COOH COO COOH COO Phospholipid: Lecithin Membranes 2nd Messengers HO + Glycerol COO HO COO HO + OPOO N
Structure of a Typical Lipoprotein Free cholesterol (surface and core) Phospholipid (amphipath at surface only) Triglyceride (core only) Cholesteryl ester (core only) Apolipoprotein (amphipath at surface only)
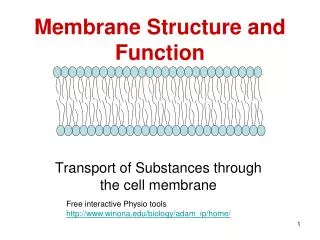
VLDL VLDL Remnants Chylomicron Remnants Directly atherogenic (found in plaque) HDL2 Lipoprotein classes and sub-Classes Chylomicron 0.95 1.006 IDL Density (g/ml) 1.02 LDL 1.06 Lp(a) 1.10 HDL3 pre-β2 HDL 1.20 pre-β1 HDL 1000 5 10 20 40 60 80 Particle Size (nm)
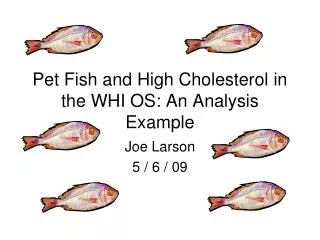
CPT I Acyl-Carnitine CPT II Substrates for Triacylglycerol Synthesis Plasma NEFA Triglycerides Glucose Acyl-CoA Synthetase Glc-6-Pase CoA Acyl-CoA Multiple steps Glucose-6-P Acyl-CoA PEPCK Mitochondria Pyruvate kinase Fatty Acid Synthase Hepatocyte Malonyl-CoA PEP Acyl-CoA Acyl-CoA Carboxylase Krebs Cycle Acetyl-CoA Citrate Pyruvate ATP Citrate Lyase Acetyl-CoA CO2 Pyruvate Citrate HMG-CoA Synthase Ketone Bodies Beta-oxidation PEP = phosphoenolpyruvate PEPCK = PEP carboxylase CPT = Carnitine palmitoyl transferase
Structures of Fatty Acids O 16:0 (palmitic) C HO O C cis-18:1 -6 (oleic) HO O trans-18:1 -6 (elaidic) C HO O C 18:2 -6 (linoleic) HO (alpha linolenic) O 18:3 -3 C HO O 20:5 -3 (EPA) C HO
Exogenous (dietary) lipid metabolism Muscle and adipose tissue Fatty acids Lipoprotein lipase Lipoprotein Lipase Apo C-II enhances and apo C-III inhibits LPL activity Chylomicron Remnant Bloodstream Plasma chylomicron Apo B and apo E are ligandsfor LDL receptor LDL (apo B,E) receptor clears Chylomicron Remnants I N T E S T I N E LDL receptor Lymphatic chylomicron Hepatocyte Liver Xenical blocks diatary fat digestion
Endogenous (hepatic) lipid metabolism Muscle and adipose tissue Fatty acids Lipoprotein lipase Lipoprotein Lipase And hepatic lipase Apo C-II enhances and apo C-III inhibits LPL activity LDL Bloodstream IDL Apo B and apo E are ligandsfor LDL receptor LDL (apo B,E) receptor clears VLDL, IDL & LDL LDL receptor VLDL Hepatocyte Liver
Clinical Hypertriglyceridaemia Condition Features Secondary Relatively common (obesity, diabetes, renal impairment, liver disease, drugs) Polygenic Accounts for the majority of cases Familial HTG TG predominates. CVD risk varies Predisposes to massive HTG Familial Overproduction of apo B lipoproteins Combined H/L TG and TC vary with age and weight Massive HTG Lipoprotein Lipase deficiency or saturation. Risk of pancreatitis
Therapy for Hypertriglyceridaemia Intervention Features Diet, Exercise Relatively responsive Alcohol restriction Often sufficient in heavy intake Manage 2o causes Diabetes, renal Fibrates Effective in high TG, low HDL Statins Mild TG and HDL benefit Fish oils (eg 6gm/d) Benefits TG rather than HDL Niacin Effective, but increases glu, urate. Future DGAT 2 Inhibitors? Bile acid resins Contraindicated. Increase TG
NORMAL CHOLESTEROL ABSORPTION 1,300 mg/day 400 mg/day Oil phase
NORMAL CHOLESTEROL ABSORPTION 1,300 mg/day 400 mg/day Oil phase Plant sterols compete with cholesterol here
NORMAL CHOLESTEROL ABSORPTION 1,300 mg/day 400 mg/day 17,400 mg/day Oil phase 850 mg/day Ezetimibe competes with cholesterol here
NORMAL CHOLESTEROL ABSORPTION 1,300 mg/day 400 mg/day 17,400 mg/day Oil phase 850 mg/day
Intracellular cholesterol sensing by SREBPs (Sterol Regulatory Element Binding Proteins) • Membrane fluidity reflects intracellular cholesterol. Low levels allow cleavage to active form which binds nuclear receptor to control gene expression. SCAP or SREBP activating protein Reg WD bHLH bHLH bHLH bHLH Reg WD Nucleus SCAP SREBP SRE ER Cytosol • SREBP-2 controls cholesterol synthesis and sterol metabolism Lumen Sterols • SREBP-1c is the major isoform in liver and is a key regulator of fatty acid & triglyceride synthesis Golgi Apparatus ZN++ S1P S2P Metalloproteinase Serine protease Other nuclear receptors: FXR, LXR.
LDL Receptor activity reflects intracellular cholesterol homeostasis Cholesterol delivery via LDL-R alters intracellular membrane cholesterol and SREBP, which Reduces synthesis via HMGCoAReductase Reduces LDL-R synthesis Increases storage as ester Reduces counter-regulatory PCSK9 *[SREBP] = sterol regulatory element-binding protein. Goldstein JL, et al. Arterioscler Thromb Vasc Biol. 2009;29:431-438..
The Role of HDL inReverse Cholesterol Transport Bile ABCG1 &SR-B1 Spheroidal HDL Pre-β HDL UC Liver LCAT ABCA1 UC Hepatic lipase, endothelial lipase PL&UC SR-BI SR-A CETP LDLReceptor Macrophage Oxidation VLDL/LDL ABCA1, ATP-binding cassette protein A1; CETP, cholesterol ester transfer protein; FC, free cholesterol; LCAT, lecithin:cholesterol acyltransferase; SR-A, scavenger receptor class A; SR-BI, scavenger receptor class B type I. Adapted with permission from Cuchel C et al. Arterioscler Thromb Vasc Biol. 2003;23:1710–1712
Clinical Hypercholesterolaemia Condition Features Secondary Relatively uncommon, but potent (hypothyroidism, nephrotic syndrome, primary biliary cirrhosis) Polygenic Accounts for the majority of cases Familial Prevalent, Accelerates CVD. Hyperchol’aemia Due to defects in genes related to LDL-R Familial Overproduction of apo B lipoproteins Combined H/L TG and TC vary with age and weight Increased HDL ?OK if LDL not raised?
Therapy for Hypercholesterolaemia Intervention Features Diet Plant sterols, avoid sat & trans FA Manage 2o causes Rarer, but potent: (Thyroid, liver, renal.) Statins First line for LDL reduction Ezetimibe 2nd line. Neutral for TG & HDL Niacin Improves LDL, TG, HDL & Lp(a) Bile acid resins Colesevalam better tolerated Future PCSK9 Inhibitors, MTP inhibitors? Apo B antisense oligonucleotides
Triglyceride and Cholesterol:Why are they linked? Most lipoproteins have TG and/or CE in their core Hepatic Triglyceride rich lipoproteins are precursors of cholesterol-rich LDL Cholesterol-ester transfer protein allows all triglyceride-rich lipoproteins to modify the composition of cholesterol-rich HDL and LDL. As a result, hypertriglyceridaemia is associated with reduced HDL cholersterol as well as “small dense LDL”. The major gene regulators for lipid metabolism affect both TG and Chol
SHP LXR PPAR RXR Key Regulators of Genes in Fatty Acid and Triglyceride Metabolism Bile Acids SHP = Short Heterodimer Partner SREBP-1c FXR Acetyl CoA Carboxylase Fatty Acid Synthase Spot 14 Acyl CoA NEFA Unsaturated Saturated HNF-4α L-FABP Fatty acid metabolism Transport Oxidation Fatty Acid Binding Protein Ketogenesis Apolipoproteins Pyruvatekinase Glucose-6-phosphalase Transferin Bile Acids Adapted from Pegorier JP et al. J Nutr 2004;134:2444S-9S
Key Regulators of Genes in Lipid Metabolism Sterol Regulatory Element Binding Protein (SREBP2) Peroxisome proliferated activator receptors PPARs Synthesis Delivery Acquisition Cellular Cholesterol Homeostasis Excretion Intestine Hepatobiliary Liver X Receptor (LXR) Farnesoid X Receptor (FXR)
Case MC Patient is a 43 year-old male with a strong family history of premature CVD who presents for initial evaluation. He has a 10 year history of dyslipidaemia and hypertension, for which he has received beta blockers in the past. More recently he has been on an ARB/diuretic combination. Three months prior to this visit a fasting lipid profile showed: Total Cholesterol: 5.7 mmol/L Triglyceride: 2.8 mmol/LHDL-C: 0.7 mmol/L LDL-C: 3.6 mmol/L He has managed to lose 3 kg and today results include: Total Cholesterol: 6.9 mmol/L Triglyceride: 1.8 mmol/L HDL-C: 0.8 mmol/L LDL-C: 5.2 mmol/L
Questions concerning Mr M.C. • 1) Is ethnicity an independent risk factor for CVD? Yes / No? • 2) In the absence of any symptoms or signs of hypothyroidism, would you perform thyroid function tests? Yes / No? • 3) His brother’s lipids include LDL = 5.4 mmol/l, TG = 1.9 mmol/l, HDL = 0.9 mmol/l . What is the most likely cause of MC’s lipid abnormality? • A) Dyslipidaemia secondary to Insulin resistance and the Metabolic Syndrome • B) Polygencdyslipidamia • C) Familial Combined Hyperlipidaemia • D) Familial Hypercholesterolaemia • E) Lipids aren’t really an issue in this patient
Patient is a 43 year-old male with a strong family history of premature CVD who presents for initial evaluation. He has a 10 year history of dyslipidaemia. Hypertension, for which he has received beta blockers in the past. More recently he has been on an ARB/diuretic combination. Three months prior to this visit a fasting lipid profile showed: TC: 5.7 Triglyceride: 2.8 mmol/L HDL-C: 0.7 mmol/L LDL-C: 3.6 mmol/L He has managed to lose 3 kg and today results include: TC: 6.9 Triglyceride:1.8 mmol/L HDL-C: 0.8 mmol/L LDL-C: 5.2 mmol/L • 1) Is ethnicity an independent risk factor for CVD? Yes / No? • 2) In the absence of any symptoms or signs of hypothyroidism, would you perform thyroid function tests? Yes / No? • 3) His brother’s lipids include LDL = 5.4 mmol/l, TG = 1.9 mmol/l, HDL = 0.9 mmol/l . What is the most likely cause of MC’s lipid abnormality? • A) Dyslipidaemia secondary to Insulin resistance and the Metabolic Syndrome • B) Polygencdyslipidamia • C) Familial Combined Hyperlipidaemia • D) Familial Hypercholesterolaemia • E) Lipids aren’t really an issue in this patient
Is ethnicity an independent risk factor for CVD? Yes / No? YES: NO:
Is ethnicity an independent risk factor for CVD? Case for a qualified “Yes”.Same risk factors, different pattern INTERHEART, Karthikeyan et al 2009, INTERHEART, Joshi et al 2007
2) In the absence of any symptoms or signs of hypothyroidism, would you perform thyroid function tests? Yes / No? Yes: No:
2) In the absence of any symptoms or signs of hypothyroidism, would you perform thyroid function tests? The case for “Yes”
What is the most likely cause of MC’s lipid abnormality? • A) Dyslipidaemia secondary to Insulin resistance and the Metabolic Syndrome • B) Polygencdyslipidamia • C) Familial Combined Hyperlipidaemia • D) Familial Hypercholesterolaemia • E) Lipids aren’t really an issue in this patient
What is the most likely cause of MC’s lipid abnormality? The case for “C”, maybe “A” or “B” Condition Features Secondary Relatively uncommon, but potent (hypothyroidism, nephrotic syndrome, primary biliary cirrhosis) Polygenic Accounts for the majority of cases Familial Prevalent, Accelerates CVD. Hyperchol’aemia Due to defects in genes related to LDL-R Familial Overproduction of apo B lipoproteins Combined H/L TG and TC vary with age and weight Increased HDL ?OK if LDL not raised?
Case MC (continued) • Mr MC started statin, therapy, Atorvastatin 20 mg/ day, but unfortunately he had and inferior AMI still 4 months later. His discuharge medication include: • Atorvastatin 20mg, Metoprolol 20 mg, Aspirin 100mg, and his previous ARB/diuretic. Follow-up 2 months later reveals: 2 kg weight loss, BP 118 / 78, Fasting tests: • Glu 5.3 mmol/l, TC 4.4 mmol/l TG 4.2 mmol/l, • HDL 0.7 mmol/l, LDL 1.8 mmol/l
Case MC: Further questions: • Should you stop his beta blocker? Yes / No? • Do you trust the LDL-C result? Yes / No? • Is it practical to try to manage Mr M.C’s lipid profile to target levels? Yes / No? • What is the next lipid-lowering drug that you would add to his therapy? • Ezetimibe • Niacin • I would increase Atorvastatin to 80 mg but I wouldn’t give anything other than a statin • Fenofibrate • Fish Oil
Mr MC started statin, therapy, Atorvastatin 20 mg/ day, but unfortunately he had and inferior AMI still 4 months later. His discuharge medication include: • Atorvastatin 20mg, Metoprolol 20 mg, Aspirin 100mg, and his previous ARB/diuretic. Follow-up 2 months later reveals: 2 kg weight loss, BP 118 / 78, Fasting tests: • Glu 5.3 mmol/l, TC 4.4 mmol/l TG 4.2 mmol/l, • HDL 0.7 mmol/l, LDL 1.8 mmol/l • Should you stop his beta blocker? Yes / No? • Do you trust the LDL-C result? Yes / No? • Is it practical to try to manage Mr M.C’s lipid profile to target levels? Yes / No? • What is the next lipid-lowering drug that you would add to his therapy? • Ezetimibe b) Niacin c) Increase Atorvastatin to 80 mg but don’t give anything other than a statin • d) Fenofibrate e) Fish Oil
Should you stop his beta blocker? • Yes • No
Should you stop his beta blocker? The case for “no” Some β-blockers decrease HDL and increase triglycerides.25 In spite of this, BHAT data showed that propranolol improves survival after MI.26 Low-dose metoprolol CR/XL alone or in combination with a statin resulted in significant slowing of the progression of carotid artery’s intima-media thickness over a 3-year period.27 M Gheorghiade et al Circulation.2002; 106: 394-398
Do you trust the LDL-C result? • Yes • No
Do you trust the LDL-C result? The case for “No” Discussion of the effect of Cholesterol ester transfer protein will Explain why LDL-C underestimates risk when TG is elevated
Is it practical to try to manage Mr M.C’s lipid profile to target levels? • Yes • No
Is it practical to try to manage Mr M.C’s lipid profile to target levels? The case for “Yes” Combination therapy is safe and effective, but yet to be supported by clinical endpoint data.
What is the next lipid-lowering drug that you would add to his therapy? • Ezetimibe • Niacin • I would increase Atorvastatin to 80 mg but I wouldn’t give anything other than a statin • Fenofibrate • Fish Oil
What is the next lipid-lowering drug that you would add to his therapy? The case for “d” or “b”, possibly “c” or “e” anticipate “residual risk” module
Case GS Patient is a 47 year-old female who has been gaining weight for several years. She has a 10 year history of mildly elevated triglyceride. She received therapeutic lifestyle counseling but she has been largely non-compliant. Three months prior to this visit, a fasting lipid profile showed: Total Cholesterol: 5.5mmol/L Triglyceride: 2.4mmol/LHDL-C: 1.0mmol/L LDL-C:3.6 mmol/L Now she has symptoms of hyperglycaemia and repeat fasting glucose confirms Type 2 diabetes
Case GS • Review of Symptoms: Thirst, polyuria, folliculitis, • Weight unchanged (increased 2kg, then lost when polyuria commenced • BP 118/72 Pulse 72 Wt 85kg Ht 175cm Waist 93 cm BMI 27.8: Physical examination unremarkable • Current fasting lipid results surprise you: • Total Cholesterol: 8.5mmol/L • Triglyceride: 7.4mmol/L • HDL-C: 1.0mmol/L • LDL-C: unable to be calculated
Questions: • How could you obtain an LDL-C result? • Friedewald equation • Abusive phonecall to lab • “Direct method” involving detergents • Ultracentifugation • Subtract HDL-C from Total cholesterol • Which class or classes of lipoproteins would you expect to be increased? • Chylomicrons and LDL • VLDL and LDL • VLDL and HDL • IDL and chylmicron “remnants” • Why bother? It doesn’t matter Which combination of extra tests would be most useful? • a) LDL size+HDLsubfractions b) Lipid EPG+ApoEphenotype c) LDL subfractions HDL size d) Lp(a)+ homocysteine • e) Routine fasting lipids are the only lipid tests that are ever required
She has a 10 year history of mildly elevated triglyceride. She received therapeutic lifestyle counseling but she has been largely non-compliant. Three months prior to this visit, a fasting lipid profile showed: Total Cholesterol: 5.5mmol/L Triglyceride: 2.4mmol/L HDL-C: 1.0mmol/L LDL-C:3.6 mmol/L Now she has symptoms of hyperglycaemia and repeat fasting glucose confirms Type 2 diabetes. Symptoms: Thirst, polyuria, folliculitis, Weight increased 2kg, then lost when polyuria commenced • BP 118/72 Pulse 72 Wt 85kg Ht 175cm Waist 93 cm BMI 27.8: Physical examination unremarkable • Current fasting lipid results surprise you: TC: 8.5mmol/L TG: 7.4mmol/L HDL-C: 1.0mmol/L • LDL-C: unable to be calculated • How could you obtain an LDL-C result? • Which class or classes of lipoproteins would you expect to be increased? • Which combination of extra tests would be most useful?
How could you obtain an LDL-C result? • Friedewald equation • Abusive phonecall to lab • “Direct method” involving detergents • Ultracentifugation • Subtract HDL-C from Total cholesterol
How could you obtain an LDL-C result? The case for “d”, but “c” is misleading Lab Tests Online: “Direct LDL-C is ordered whenever calculation of LDL cholesterol will not be accurate because the person's triglyceridesare significantly elevated. It may be ordered by a doctor when prior test results have indicated high triglycerides. In some laboratories, this direct LDL test will automatically be performed when the triglyceride levels are too high to calculate LDL-C. This saves the doctor time by not needing to order another test, saves the patient time by not needing to have a second blood sample drawn, and speeds up the time to provide the test result.” Ultracentrifuge gives absolute result. Detergent methods assume LDL
Which class or classes of lipoproteins would you expect to be increased? • Chylomicrons and LDL • VLDL and LDL • VLDL and HDL • IDL and chylmicron “remnants” • Why bother? It doesn’t matter