Download
1 / 1
10 likes | 202 Views
Analysis of Cardiovascular Risk Factors in the HIV Outpatient Study (HOPS) Cohort. #735. Kenneth A. Lichtenstein, MD University of Colorado Health Sciences Center 4200 East 9 th Avenue, B163 Denver, Colorado, 80262 Kenneth.Lichtenstein@uchsc.edu P - 303-320-2830 F - 303-320-7016.

E N D
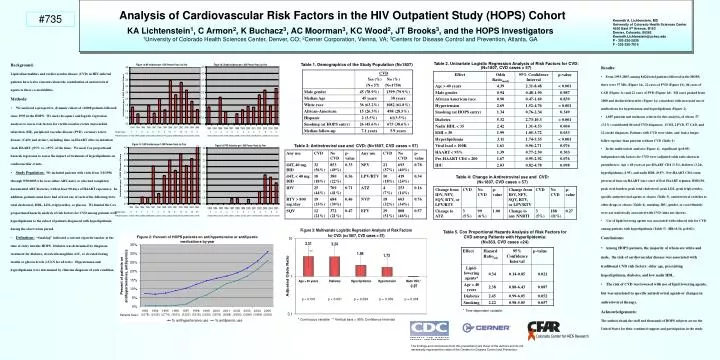
Analysis of Cardiovascular Risk Factors in the HIV Outpatient Study (HOPS) Cohort #735 Kenneth A. Lichtenstein, MD University of Colorado Health Sciences Center 4200 East 9th Avenue, B163 Denver, Colorado, 80262 Kenneth.Lichtenstein@uchsc.edu P - 303-320-2830 F - 303-320-7016 KA Lichtenstein1, C Armon2, K Buchacz3, AC Moorman3, KC Wood2, JT Brooks3, and the HOPS Investigators 1University of Colorado Health Sciences Center, Denver, CO; 2Cerner Corporation, Vienna, VA; 3Centers for Disease Control and Prevention, Atlanta, GA • Background: • Lipid abnormalities and cardiovascular disease (CVD) in HIV-infected patients have led to concerns about the contribution of antiretroviral agents to these co-morbidities. • Methods: • We analyzed a prospective, dynamic cohort of >8,000 patients followed since 1993 in the HOPS. We used chi-square and logistic regression analyses to assess risk factors for cardiovascular events (myocardial infarction (MI), peripheral vascular disease (PVD), coronary artery disease (CAD) and stroke), including time on HAART after its initiation (took HAART >95% vs. <95% of the time). We used Cox proportional hazards regression to assess the impact of treatment of hyperlipidemia on cardiovascular events. • Study Population: We included patients with visits from 3/1/1996 through 9/30/2005 who were either ARV-naïve or who had completely documented ARV histories, with at least 90 days of HAART experience. In addition, patients must have had at least one of each of the following tests: total cholesterol, HDL, LDL, triglycerides, or glucose. We limited the Cox proportional hazards analysis of risk factors for CVD among patients with hyperlipidemia to the subset of patients diagnosed with hyperlipidemia during the observation period. • Definitions: “Smoking” indicated a current cigarette smoker at the time of entry into the HOPS. Diabetes was determined by diagnosis, treatment for diabetes, elevated hemoglobin A1C, or elevated fasting insulin or glucose levels (>ULN for all tests). Hypertension and hyperlipidemia were determined by clinician diagnosis of each condition. Table 1. Demographics of the Study Population (N=1807) Table 2. Univariate Logistic Regression Analysis of Risk Factors for CVD: (N=1807, CVD cases = 57) • Results: • From 1993-2005, among 8,024 total patients followed in the HOPS, there were 57 MIs (Figure 1a), 22 cases of PVD (Figure 1b), 86 cases of CAD (Figure 1c) and 22 cases of PVD (Figure 1d). MI cases peaked from 2000 and declined thereafter (Figure 1a) coincident with increased use of medications for hypertension and hyperlipidemia (Figure 2). • 1,807 patients met inclusion criteria for this analysis, of whom 57 (3.2%) contributed 84 total CVD diagnoses: 13 MI, 2 PVD, 57 CAD, and 12 stroke diagnoses. Patients with CVD were older, and had a longer follow-up time than patients without CVD (Table 1). • In the multivariate analysis (Figure 4), significant (p<0.05) independent risk factors for CVD were (adjusted odds ratio shown in parentheses): Age > 40 years at pre-HAART CD4 (3.31), diabetes (3.24), hyperlipidemia (1.95), and nadir HDL (0.97). Pre-HAART CD4 count, percent of time on HAART since start of first HAART regimen, BMI>30, peak viral burden, peak total cholesterol, peak LDL, peak triglycerides, specific antiretroviral agents or classes (Table 3), antiretroviral switches to other drugs or classes (Table 4), smoking, IDU, gender, or race/ethnicity were not statistically associated with CVD (data not shown). • Use of lipid-lowering agents was associated with reduced risk for CVD among patients with hyperlipidemia (Table 5) (HR=0.34, p=0.02). • Conclusions: • Among HOPS patients, the majority of whom are white and male, the risk of cardiovascular disease was associated with traditional CVD risk factors: older age, preexisting hyperlipidemia, diabetes, and low nadir HDL. • The risk of CVD was lowered with use of lipid lowering agents, but was unrelated to specific antiretroviral agents or changes in antiretroviral therapy. • Acknowledgements: • The authors thank the staff and thousands of HOPS subjects across the United States for their continued support and participation in the study. Diagnoses: 1 1 0 3 2 5 3 10 7 10 8 5 2 1 0 4 2 0 2 3 4 4 7 8 4 5 Patients seen: (1070)(1949)(2530)(2742)(3062)(3070)(3175)(3435)(3454)(3483)(3427)(3164) (2724) (1061)(1935)(2519)(2746)(3043)(3048) (3157)(3410)(3439)(3473) (3428)(3173)(2737) Table 3: Antiretroviral use and CVD: (N=1807, CVD cases = 57) Table 4: Change in Antiretroviral use and CVD: (N=1807, CVD cases = 57) Diagnoses: 0 0 1 1 7 2 6 10 8 12 9 10 20 0 0 0 0 1 1 0 1 0 3 7 6 3 Patients seen: (1064)(1937)(2508)(2708)(3031)(3021)(3132)(3382)(3413)(3442)(3394)(3140) (2719) (1063)(1942)(2522)(2707)(3051) (3055) (3165) (3417)(3446)(3479) (3436)(3177)(2737) Table 5. Cox Proportional Hazards Analysis of Risk Factors for CVD among Patients with Hyperlipidemia: (N=363, CVD cases =24) ** p < 0.001 p < 0.001 p = 0.024 p = 0.059 p = 0.004 * Time-dependent variable. Patients Seen: * Continuous variable ** Vertical bars = 95% Confidence Intervals The findings and conclusions from this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.