Download
1 / 19
220 likes | 526 Views
VTE Prophylaxis Focus on Prevention. Deep Vein Thrombosis. Deep vein thrombosis (DVT) forms in a vein of the leg. Characterized by pain, swelling or tenderness of the leg, sometimes with redness and warmth. Pulmonary embolism.

E N D
VTE Prophylaxis Focus on Prevention
Deep Vein Thrombosis Deep vein thrombosis (DVT) forms in a vein of the leg. • Characterized by pain, swelling or tenderness of the leg, sometimes with redness and warmth
Pulmonary embolism • Pulmonary embolism (PE) occurs when the blood clot breaks loose and travels to the lungs • Characterized by shortness of breath, sharp rib/chest pain and occasionally by hemoptysis, light-headedness, or collapse
Symptoms and Signs of DVT • Leg pain (90%) • Tenderness (85%) • Ankle edema (76%) • Calf swelling (42%) • Dilated veins (33%) • Dusky discoloration (30%) • Warmth • Redness Most hospitalized patients with DVT will have NO SYMPTOMS or SIGNS! DVT cannot be reliably diagnosed on the basis of history and physical exam, even in high-risk patients. Symptomatic DVT
Risk of VTE in Hospitalized Patients Geerts WT, et al. Chest 2008;358:381S-453S.
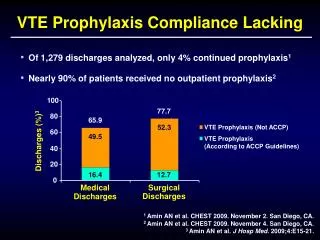
Pulmonary Embolism Hospital Risk • Accounts for 10% of hospital deaths • In the UK, PE following DVT causes between 25,000 and 32,000 deaths each year1 International, cross-sectional audit of 35,000 inpatients at risk for VTE found:2 • only 59% of surgical patients and 40% of medical patients received recommended prophylaxis. • UK House of Commons Health Committee. HC 99. Published on 8 March 2005. • Cohen AT, et al. Lancet 2008;371:387-394.
Characterization of VTE events In the Worcester County, Mass VTE Study • 60-70% of VTE events were considered to be provoked by: • Recent hospitalization (within 3 months) • Surgery • Trauma/fracture • Pregnancy Risk for VTE increases with the number of risk factors and persists after hospital discharge. Spencer FA, et al. Arch Intern Med 2007;167:1471-5. Spencer FA, et al. J Thromb Thrombolysis 2009;28:401-9.
Marco’s Story • Video clip to be embedded here
The risk of DVT and PE is increased by several factors, including: Adapted from: Greer IA. Bailliere’s Clin Obstet Gynaecol 1997;11:403-30.
VTE iscommon in hospital patients VTE isfatal (acutely and long-term) VTE ispreventable(safely and inexpensively) Preventing VTE is the standard of carefor almost all hospital patients in 2011 Rationalefor Thromboprophylaxis Slide courtesy of Dr. William Geerts.
Adverse Consequences of VTE $ Slide courtesy of Dr. William Geerts.
Key steps to ensure compliance with ROP: • Written policy/guideline • Identifies clients at risk & provides VTE prophylaxis • Establishes measures of success, uses information to make improvements • Provides information to health professionals (on risks & prevention measures)
Audrey’s Story Following a one week wait for surgery and the successful removal of a benign tumour – Audrey developed a PE. We are scared and worried about our surgery or primary reason for being in the hospital as it is. We rely on you to make us aware of any possible complications. For me, the blood clot was far scarier and worse than my brain tumour and operation. This experience with the blood clot has impacted my life. It was the scariest and worst experience I have ever had and it has left me fearful and anxious. • “My plea to healthcare professionals: make sure you get people’s attention, and make sure they fully understand their risks and what can be done to prevent a blood clot.”
Guidelines for Prevention of VTE *Use clinical judgment to weigh the risk of venous thromboembolism versus the risk of bleeding.
Prevention of VTE in Hospitalized Patients: Summary of Good Practice Tinzaparin dosing considerations according to weight • 50-100 kg: tinzaparin 4 500 units sc once a day • <50 kg: tinzaparin 3 500 units sc once a day Clinical order sets for a predominately obese population may warrant two or three weight ranges using prefilled syringe sizes. • 100-150 kg: tinzaparin 10 000 units sc once a day • 151-200 kg: tinzaparin 14 000 units sc once a day
Use of LMWHs in Renal Impairment • Due to differences in LMWH molecule size and charge, longer chained and more charged LMWHs like tinzaparin do not appear to require dose adjustments in patients with: • impaired renal function1 • renal failure2,3 • on haemodialysis2,3 • Dose reduction may be necessary with shorter chain LMWHs (i.e. enoxaparin) Mahé O, et al.Thromb Haemost 2007;97:581-6. PROTECT Investigators. N Engl J Med 2011;364:1305-14. Nutescu EA, et al. Ann Pharmacother 2009;43:1064-83.
Every in-patient w/o contraindication should be on VTE Prophylaxis