Download
1 / 17
170 likes | 402 Views
BIOE 220/rad 220 Review session 8. March 19, 2012. What We’ll Cover Today. Comments on homework 6 Anatomy leftover review Physics leftover review Questions Reminder: check the fourth review session slides for some exam preparation material. Common Issues on HW 6.

E N D
BIOE 220/rad 220 Review session 8 March 19, 2012
What We’ll Cover Today • Comments on homework 6 • Anatomy leftover review • Physics leftover review • Questions • Reminder: check the fourth review session slides for some exam preparation material
Common Issues on HW 6 • Problem 22 asked if the CBF was higher or lower at the occluded vessel • The difference values were more negative, but the magnitude of the difference indicates CBF, so it was higher • ASL (arterial spin labeling) tags spins in the neck arteries, and then images them in the head • If vessels are flowing slowly, we won’t see them in the head since they won’t have arrived yet when the rest of the arterial blood does • VSASL does not have this problem, so it sees slow flow • Problem 24 stated “In fMRI, you get about a 1% signal intensity change for about a 50% change in CBF” • As we discussed in a previous homework, blood only accounts for about 4% of the brain tissue volume, so even large relative changes in the blood will be small overall
New physics material since the midterm • MRI: • Scan time to acquire Ny phase encodes: Ny*TR • Number of slices we can interleave during acquisition: floor(TR / (time from 90º pulse to the end of sampling) ) • How is MR image reconstructed? 2D Fourier Transform • Ultrasound: • Doppler shift: fshift= 2 * (v/c) * f0 * cos(θ) • Pulsed doppler gives velocity spectrum at particular point • Color doppler overlays doppler information as color (be aware of doppler aliasing) • Hope to measure whether >70% stenosis exists in carotid • Adult transcranialdoppler ultrasound can be acquired transorbital, transtemperal, transforaminal
New physics material since the midterm • MRI Sequences: • Understand how gradients relate to k-space trajectory • Be able to relate pulse sequence diagram to acquisition type (GRE, SE, Spatial Saturation, Fat Sat (Chem Sat or STIR), FLAIR, Flow Encoding, Diffusion, Fast Spin Echo, Spiral, EPI) • Perfusion: • CBF (Cerebral Blood Flow): Rate at which blood flows through tissue • CBV (Cerebral Blood Volume): Volume of blood in brain • MTT (Mean Transit Time): Average amount of time it takes particles to move through a voxel OR Average amount of time it takes injected contrast to reach ROI • Diffusible contrast agents cross the BBB (i.e. breathing Xenon)
New physics material since the midterm • Perfusion: • Arterial spin labeling (ASL) takes two images of the head, one normal, one with the neck “tagged” prior to imaging so that arterial blood will have lower signal. Difference image represents CBV • Longer delay time gives better quantitation, but lower SNR • Isn’t sensitive to slow flow • VSASL is a similar measure that won’t miss slow vessels • Both approaches are non-contrast • CT Perfusion measures the signal response to contrast bolus injection • Can infer MTT, CBV, CBF from the shape and timing of the response • Stroke area takes a longer time to reach max contrast, Tmax > 6 seconds • If CBF/CBV has also reduced noticeably, tissue is already dead • Review the “Pros/Cons” of the different methods
New physics material since the midterm • fMRI: • Brain is only 2% of body weight, but uses 15% of cardiac output and 20% of body energy • When neurons are active, they need energy to restore equilibrium (must be resupplied with additional blood) • CMRO2 = OEF * [O2]a* CBF • CMRO2 = Cerebral metabolic rate of oxygen • OEF = oxygen extraction factor • [O2]a = Arterial oxygen constant • All parameters change with neural activation except [O2]a • Contrast agent methods exploit changes in CBV • BOLD measures changes in T2* induced by changes in oxygenation state of hemoglobin • Block design: Alternate periods of task/no task, and measure the changes in brain signal between the two stages
Spinal Cord Anterior Right Left Posterior
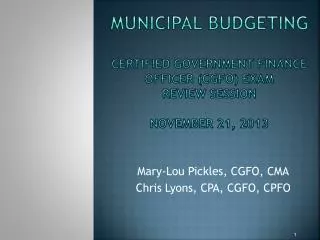
Spinal Column Basic plans of (A) posterior column-medial lemniscal pathway; (B)spinothalamic pathway.
Spinal Column • Poster columns medial lemniscus (PCML) • Touch • Spinothalamic • Pain • Temperature • 3 neuron system • Both cross the midline • Pcml near sensory decussation in medulla • ST at or near the level of entry • All involve the thalamus • Project to postcentralgyrus
Spinal Column • Corticospinal tract • Voluntary motion • Two neuron system • Precentralgyrus through motor decussation (medulla) to contralateral anterior horn • Anterior horn gray matter to muscle
Myelogram • Myelography is an imaging test that uses a special dye to view the spinal cord. Along with an x-ray , the dye can help your doctor clearly outline the space containing the spinal cord, nerves, to show any disk herniation. • Myelography is used to detect problems in and around the spinal cord. The problems that may be causing ongoing pain that has not been relieved by medication, physical therapy, and activity modification. Myelography can detect issues such as: • Spinal tumors • Spinal cord swelling • Herniated disks • Narrowing of the spinal canal due to spinal stenosis
Thank You • Please Remember to fill out TA evaluations • The rest of the time will be available for questions