Download
1 / 30
360 likes | 748 Views
LUNG VOLUMES & CAPACITIES. Lecture-3 Dr.Zahoor Ali Shaikh. Lung Volumes. Tidal Volume [TV] It is volume of air we breathe in or breathe out during single normal breath. It is about 500ml. Inspiratory Reserve Volume [IRV]

E N D
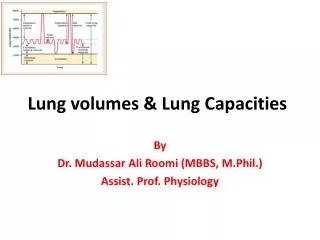
LUNG VOLUMES & CAPACITIES Lecture-3 Dr.Zahoor Ali Shaikh
Lung Volumes • Tidal Volume [TV] It is volume of air we breathe in or breathe out during single normal breath. It is about 500ml. • Inspiratory Reserve Volume [IRV] • It is volume of air that can be breathed in [inspired] forcefully, over and above normal tidal volume. • IRV is about 3000ml. • It is done by maximal contraction of diaphragm, external inter-costal muscles and accessory muscles of inspiration.
Lung Volumes • Expiratory Reserve Volume [ERV] • It is maximum volume of air that can be expired forcefully after normal tidal expiration. • ERV is about 1000ml. • It is done by contracting the accessory expiratory muscles of expiration [abdominal and internal-intercostal muscles].
Lung Volumes • Residual Volume ( RV ) • It is volume of air remaining in the lungs after maximal expiration. • RV is about 1200ml.
Lung Capacities • Inspiratory Capacity [IC] • It is maximum volume of air that can be inspired after normal tidal expiration. • It includes tidal volume and inspiratory reserve volume. • (IC = IRV + TV) • It is about 3500ml.
Lung Capacities • Functional Residual Capacity [FRC] • It is volume of air that remains in the lungs after normal tidal expiration. • (FRC = ERV + RV) • Average value FRC = 2200ml.
Lung Capacities • Vital Capacity [VC] • It is maximum volume of air that can be expired forcefully after taking maximum inspiration [during a single breath]. • (VC = IRV + TV + ERV) • Average value VC = 4500ml.
Lung Capacities • Total Lung Capacity [TLC] • It is the maximum volume of air that the lungs can hold. • (TLC = TV + IRV + ERV + RV) • Average volume TLC = 5700ml [5.5-6 liter]. • TLC is affected by Age, Build, Height and Weight, and presence of Lung disease.
Forced Expiratory Volume In One Second [FEV1] • Forced Expiratory Volume • It is volume of air that can be expired forcefully during the first second of expiration [normally we expire in 3sec]. • FEV1 = 80% [80% of vital capacity(VC)] • FEV2 = 92% • FEV3 = 99% • FEV1 indicates maximal air flow rate from the lungs. • FEV1 is decreased in obstructive lung disease e.g. bronchial asthma.
Respiratory Diseases • Obstructive Lung Disease e.g. bronchial asthma. • Restrictive Lung Disease e.g. pulmonary fibrosis. • Obstructive Lung Disease • Patient has difficulty in expiration [due to obstruction of bronchi]. • Therefore, FEV1 and FEV1% is decreased. • Example: Normal VC = 5 liters, FEV1 = 4 liters. • FEV1% = (FEV1/FVC) * 100 = (4/5) * 100 = 80% • In Obstructive Lung Disease, VC = 4 liters, FEV1 = 2 liters • FEV1% = (2/4)*100 = 50%
Respiratory Diseases • Restricted Lung Disease • Lungs are smaller than normal, therefore, vital capacity[VC], TLC, all are decreased as lungs can not expand. • When we do respiratory function test: • FEV1 is decreased, FVC is also decreased but FEV1% is normal [80% or more]. • Example: Normal VC = 5 liters, FEV1 = 4 liters. • FEV1% = (FEV1/FVC) * 100 = (4/5) * 100 = 80% • In Restricted Lung Disease, VC = 3 liters, FEV1 = 2.7 liters • FEV1% = (2.7/3)*100 = 90%
Pulmonary Ventilation & Alveolar Ventilation • Pulmonary Ventilation or Minute Ventilation • It is volume of air we breathe in and out in 1min. • Pulmonary Ventilation = Tidal Volume * Respiratory rate = 500ml * 12= 6000ml or 6 liter • Normal respiratory rate is 12 -18/min. • Adult young person can increase pulmonary ventilation 25-fold to 150 liters/min [to increase pulmonary ventilation one has to increase tidal volume and respiratory rate].
Anatomic Dead Space • As we breath in, all air does not go to alveoli for gas exchange but some of the air remains in trachea and bronchi [conducting zone] and does not take part in gas exchange. • It is 150ml. It is called ‘Anatomic Dead Space’. • As our tidal volume is 500ml, anatomic dead space is 150ml, therefore, 350ml goes to lungs for gas exchange.
Alveolar Ventilation • It is volume of air reaching the alveoli/min. • It is more important than pulmonary ventilation. • It is alveolar air that takes part in gas exchange. • Alveolar Ventilation = TV – Dead Space * Respiratory Rate[RR] = (500 – 150) * 12 = 350 * 12 = 4200 ml/min • Alveolar Ventilation is less than Pulmonary Ventilation.
Effect of Breathing Pattern on Alveolar Ventilation • Rapid shallow breathing is not good, as TV is decreased and most of the air is lost in dead space and little or no air goes to alveoli. • Person may get unconscious within few minutes.
Alveolar Dead Space • Normally air going into the alveoli, takes part in gas exchange, therefore, there is no alveolar dead space in healthy person. • In case of disease, where alveoli are abnormal e.g. pneumonia, gas exchange does not take place in affected alveoli, therefore, alveolar dead space is there. • Physiological Dead Space = Anatomical Dead Space + Alveolar Dead Space
Dead Space • In Health, Physiological dead space=Anatomical dead space [As all alveoli are functioning]. • In Disease, Physiological dead space is more than Anatomical dead space [As many alveoli are not functioning].
Ventilation and Perfusion in the Lungs • Regional difference exist at the top and bottom [apex and base] of the lung due to gravitational effect. • Standing upright • Gravity effect is more on blood flow than on airflow. • Effect on Ventilation/Perfusion ratio.
Ventilation and Perfusion in the Lungs • Top of the lung receives relatively more air than blood, therefore, ventilation perfusion ratio is increased. • Bottom of the lung receives relatively less air than blood, therefore, ventilation perfusion ratio is decreased.
Important Points • During normal breathing, lungs are not totally full nor totally deflated. • At the end of normal quiet expiration, the lungs contain about 2200 ml of air. • Lungs can never be completely emptied therefore gas exchange can take place after forceful expiration.
What You Should Know From This Lecture • Lung volumes – TV, IRV, ERV, RV • Lung capacities – IC, FRC, VC, TLC • FEV1, FEV1% and their importance in Obstructive and Restrictive Lung Disease • Alveolar Ventilation & Pulmonary Ventilation • Anatomic Dead Space • Physiological Dead Space • Ventilation Perfusion at the Apex and baseof the lung