Download
1 / 40
430 likes | 936 Views
Shoulder Dystocia. PeriGen Webinar September 13, 2011. Our Agenda Today. The Clinician’s Conundrum Another Approach Case Presentations: “ What would you do?” Practical Considerations Prospective Use Results to-Date PeriCALM Tracings and Tracing Analysis . “Clinicians Conundrum” .

E N D
Shoulder Dystocia PeriGen Webinar September 13, 2011
Our Agenda Today • The Clinician’s Conundrum • Another Approach • Case Presentations: “ What would you do?” • Practical Considerations • Prospective Use Results to-Date • PeriCALM Tracings and Tracing Analysis
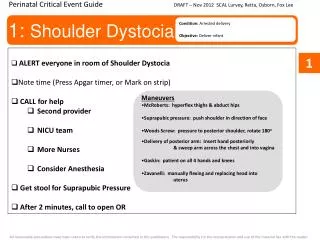
Clinician’s Dilemma:ACOG Shoulder Dystocia Risk Factors and Intervention Guidelines • Some ACOG Risk Factors Are Present • in Almost ALL Births • Macrosomia (> 4000g) • Maternal Diabetes • Obesity • Multiparity • Post Dates • Previous Shoulder Dystocia • Previous Macrosomia • Induction of Labor • Epidural Anesthesia • Operative Vaginal Delivery • ACOG Intervention Present in Very few • Consider Cesarean delivery: • Est. Fetal Wt. (EFW) > 4500g with Diabetes • Est. Fetal Wt. (EFW) > 5000g without Diabetes • Possibly with Past History of Shoulder Dystocia
Nonspecific Risk Factors / Stringent Intervention CriteriaMothers with and without Shoulder Dystocia
Case Presentation #1 Background: • 25 y/o G1 at 40 5/7 wks • For induction re: post-dates • EFW 3900g • GDM well controlled on diet • Height: 5”2”; 155 lbs now • Max fundal height 39 cm • Weight gain 45 lbs • Cervix 2cm / 75% / Station -1
Question #1 • Regarding the potential of Shoulder Dystocia in this case (G1, 40 5/7wks, EFW3900, 5’2”, 155lbs, GDM), I would: Options: • Not discuss it at this point, because risks are low • Discuss it before starting this induction • Discuss it only if first stage labor progress were slow • Discuss it only if Vacuum extraction were needed
A Different Approach to the Problem . . . • Shoulder dystocia with injury –notshoulder dystocia at large • Multiple factors – not a single factor • Interactionof maternal and fetal size – not simply additive
Distribution of Birth Weight: Vaginal Deliveries w/o Shoulder Dystocia vs. SD with pBPI PeriCALM Shoulder Screen Risk Score Distribution: Vaginal Deliveries w/o Shoulder Dystocia vs. SD with pBPI
PeriCALM Shoulder Screen in Prenatal Care 4 Simple Steps During Office Visit Step 1. Checklist at 36 weeks Step 2. Data Entry for Women with Risk Factors
PeriCALM Shoulder Screen in Prenatal Care 4 Simple Steps During Office Visit Step 3.Obtain Risk Assessment Step 4. Discuss & Document Informed Consent
Case Presentation 125 y/o G1, 40 5/7 wk, GDM, EFW 3900, 5’2”, 155Lbs, induction planned
Case Presentation 2 • 3 years later • 28 y/o G2P1 • SRM at 39 wks • EFW 4100, • Now 195 lbs, GDM controlled on diet • Previous SVD 4000g, No SD
Question #2 Regarding the potential of Shoulder Dystocia in this case (G2, 39wk, EFW4100g, GDM, 195lbs, H/O SVD 4000g), I would: Options: • Not discuss it at this point, because risks are low • Discuss it before starting this induction • Discuss it only if first stage labor progress were slow • Discuss it only if Vacuum extraction were needed
Case Presentation 228 y/o G2P1, SRM at 39 wks EFW 4100, now 195lbs, GDM controlled on diet, EFW 4100, previous SVD 4000g, No SD
PeriCALM Shoulder ScreenProspective Use Results • Is the Program Feasible? • Did We Cause Harm? • CS rates • Did We Help? • Shoulder Dystocia rates • Shoulder Dystocia with Injury Rates
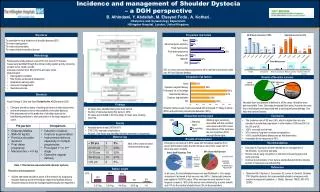
Prospective UseSecond Large Outcome Study • Opportunity to track outcome on all births across a large hospital system • EMR – PeriBirth® – in the hospital and PeriCALM Shoulder Screen™ in some physicians’ offices
Characteristics of Study Population • 20,725 Singletons at 36 weeks or greater • 8,767 With providers enrolled in formal risk assessment program • 11,958 with providers not enrolled • Total CS rate 38.6% • Primary 21.1% Repeat 17.6% • Shoulder Dystocia (216 cases, all pediatric records reviewed) • Per all births 1.0% • Per vaginal birth 1.7% • Complicated SD (SD with Any of the following : BPI, Intubation, Bag and Mask ventilation, Fracture)
Trend Analysis for Enrolled Clinicians “Complicated SD” Any SD with BPI or Fracture or Intubation or Bag and Mask Ventilation
PeriCALM Shoulder ScreenProspective Use Results • Is the Program Feasible? Yes • Did We Cause Harm? NO • Primary CS rates was stable • Did We Help? • Yes, Shoulder Dystocia rates - Decreasing • Complicated Shoulder Dystocia – looks very interesting, not yet statistically significant • Persistent BPI will required many many years
Shoulder Dystocia Risk Reduction ProgramIncludes CME Courses
Questions Contact: www.PeriGen.com
Electronic Fetal Monitoring • Real time at the point of care • Based on NICHD definitions • Unbiased, continuous analysis • Unaffected by operator inexperience, fatigue, distractions Computerized Analysis of Electronic Fetal Monitoring Peri CALM Patterns
Uterine Tachysystole Visual Alerts when excessive contraction rates occur and persist beyond acceptable limits Computerized Analysis of Contraction Rate PeriContractility Index
Labor Progression • Shows how cervical dilation is progressing • Expected range is adjusted for conditions that change during labor • Consistent • Quantifiable • VBAC , identified 42% rupture cases hours before delivery • Relevant in assessing cesarean rates Computerized Analysis of Labor Progression PeriCALM Curve
Discussion Contact: www.PeriGen.com
PeriCALM Shoulder Screen in Prenatal Care Top Allegations Are Addressed Risk Factors Were Not Recognized Patient Uninformed of Her Own Risk Patient Not Given Choice of Delivery Method No Documentation of Informed Consent • Faulty Delivery Technique
Shoulder Dystocia Risk Reduction ProgramAdditional Benefits • Potential Financial benefit • Liability insurance premium reduction • Special recognition as forward thinking advocates for mothers
CS rate 34 - 37% 8000 • SD rate 1.5% - 1.0% 15,500 • SD with any injury 0.25%-0.125 37,500 • SD with persistent BPI 0.015% -0.0075% 650,000
Peri CALM Shoulder Screen Shoulder Dystocia • Personalized estimate of risk of shoulder dystocia with BPI • Based on multiple factors • Communicate graphical and actual numerical estimate • Identifies 4 to 5 times more that standard methods • Easy to use - no special equipment required Computerized Assessment of Risk Of Shoulder dystocia with Brachial Plexus Injury
Trend Analysis for Enrolled Clinicians “Complicated SD” Any SD with BPI or Fracture or Intubation or Bag and Mask Ventilation