Download

1 / 51
510 likes | 686 Views
Towards a non-invasive approach to EGDT Daniele Coen Ospedale Niguarda Ca’ Granda - Milano. 1 - EARLY. Emanuel Rivers , Bryant Nguyen, Suzanne Havstad, et al. Early goal-directed treatment in severe sepsis and septic shock. New England Journal of Medicine 2001;345:1368-1377.

E N D
Towards a non-invasive approach to EGDT Daniele Coen Ospedale Niguarda Ca’ Granda - Milano
Emanuel Rivers, Bryant Nguyen, Suzanne Havstad, et al. Early goal-directed treatment in severe sepsis and septic shock. New England Journal of Medicine 2001;345:1368-1377. Donnino MW, Bryant Nguyen, Gordon Jacobsen, Michael Tomlanovich,Emanuel Rivers. Cryptic septic shock: a subanalysis of early goal directed therapy. Chest 2003;124:90s
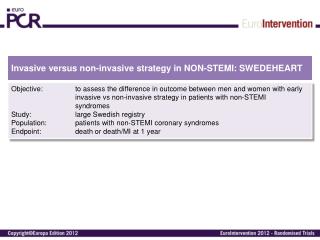
Emanuel Rivers, Bryant Nguyen, Suzanne Havstad, et al. Early goal-directed treatment in severe sepsis and septic shock. New England Journal of Medicine 2001;345:1368-1377. Inclusion criteria: Fulfillment of two of four criteria for the systemic inflammatory response syndrome AND A systolic blood pressure no higher than 90 mmHg (after a crystalloid fluid challenge of 20 to 30 ml per kilogram of body weight over a 30-minute period) OR A blood lactate concentration of 4 mmol per liter or more
O2 + intubazione OT e ventilazione meccanica CVC e catetere arterioso colture Cristalloidi CVP Colloidi 8-12 mmHg <65 Agenti vasoattivi Antibiotico MAP >90 Protocol for Early Goal-Directed Therapy Rivers, N Engl J Med 2001 >65, <90 mmHg <70% ScvO2 GRC: Ht>30% inotropi <70% >70% >70% Obiettivi raggiunti Ricovero Ospedaliero
Standard therapy 60 EGDT 50 40 Mortality (%) 30 20 10 0 In-hospital mortality 28-daymortality 60-day mortality The Importance of Early Goal-Directed therapy 46,5 30,5 Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345:1368-1377
During the initialsixhours, the patientsassigned toearlygoal-directedtherapyreceivedsignificantly more fluidthanthoseassignedto standard therapy (P<0.001) and more frequentlyreceivedred-celltransfusion (P<0.001) and inotropicsupport (P<0.001), During the periodfrom 7 to 72 hours, however, the patientsassignedto standard therapyreceivedsignificantly more fluidthanthoseassignedtoearlygoal-directedtherapy(P=0.01) and more oftenreceivedred-celltransfusion (P<0.001) and vasopressors (P=0.03) During the overallperiodfrom base lineto 72 hoursafter the start of treatment, therewas no significantdifferencebetween the twogroups in the total volume offluidadministered(P=0.73) or the rate ofuseofinotropicagents (P=0.15),
Fluid resuscitation alone can help to reduce the global tissue hypoxia that is central to the development of multiorgan dysfunction, by increasing the cardiac output and improving oxygen delivery to the tissues. Haupt MT,et al. Am Rev Respir Dis 1985;131:912–16.
EGDT issimply a protocolderivedfromcomponentsthathave long beenrecommendedas standard care for the septicpatient in the settingof the ICU. The noveltyofthisprotocolisthatitisappliedinitially at patientpresentationinsteadof at ICU admission. Therefore, EGDT wasnotanemergencydepartment (ED) study or therapy; itwas a studythatprovided “best care” to the sepsispatientasearlyaspossible. Thishappenedtobe in the ED Rivers E. Chest 2006
Knowledge translation in clinical medicine refers to the transfer of high-quality research evidence into effective changes in clinical decision-making and patient management. The failure to translate new knowledge into clinical practice is a major barrier to human benefit from biomedical researchevidence. Jones AE, et al. Acad Emerg Med 2007; 14:1072–1078
Translating Research to Clinical Practice A 1-Year Experience With Implementing Early Goal-Directed Therapy for Septic Shock in the Emergency Department* Stephen Trzeciak, MD, R. Phillip Dellinger, MD, FCCP, Nicole L. Abate, MD, Robert M. Cowan, MD, Mary Stauss, RN, J. Hope Kilgannon, MD, Sergio Zanotti, MD and Joseph E. Parrillo, MD, FCCP Chest 2006;129:225-32
The primary aim of this study was to determine if EGDT end points could reliably be achieved in real-world clinical practice. We found that all EGDT end points (CVP, MAP, and Scvo2) were successfully achieved in 20 of 22 EGDT cases (91%). The median times to achievement of each end point were ≤ 6 h. We believe that the times to successful end point achievement in this study reflect what can realistically be expected in the first year of EGDT implementation, and could be reasonably extrapolated to most academic centers. Our data demonstrates that EGDT is not just a research innovation but also a viable clinical practice parameter that can be successfully built into the armamentarium of severe sepsis care for the ED. Trzeciak S, Chest 2006
Finally, we should note that all of the authors of this report are in agreement that the implementation of EGDT at their respective institutions has resulted in improved patient care and outcomes among patients with sepsis. However, this benefit should be taken in the context of the knowledge that all of the authors are describing the clinical effectiveness of the protocol and thus are unable to definitively describe the number of patients who qualified for the protocol but were not enrolled and the number of patients who received EGDT who were actually not septic. Jones AE, et al. AcadEmerg Med 2007; 14:1072–1078
Table 1 Baseline characteristics of patients during audit period compared with early goal-directed therapy Authors’ sepsis audit Rivers EGDT (control) No of patients (period) 75 (1 year) 130 (3 years) (133) Mean age 61.8 67.4 (67.1) Mean APACHE II 18.3 16.0 (17.6) In-hospital mortality (%) 42.6 30.5(46.5) Reuben, et al. Emerg Med J 2006;23:828–832
Table 2 Resuscitation during first 6 h of audit period compared with early goal-directed therapy First 6 h of care Authors’ sepsisauditRivers EGDT (n = 59) (n = 130) Antibiotics given in the ED (%) 70 86 Mean fluid resus in ml (SD) 2970 (1918) 4981 (2438) CVP monitoring in ED (%) 22.5 100 Vasopressor in ED (%) 7.4 27.4 Red celltransfusion (%) 0 64.1 Time in ED (mean) 4:50 8:00 Reuben, et al. Emerg Med J 2006;23:828–832
In this single-center cohort study, we found that EGDT was not initiated in 42% of eligible patients and was incomplete in 43% of patients in whom EGDT was initiated. We identifi ed potential barriers to the initiation of EGDT at the patient, clinician, and organizational level. Our findings demonstrate the challenges that exist in translating evidence into clinical practice effectively. Despite evidence that adoption of EGDT led to improved outcomes at our institution, EGDT was underused. Mikkelsen, et al. Chest 2010
Many intensivists and emergency medicine physicians balk at inserting central venous catheters to comply with a protocol when their clinical gestalt tells them the catheter is unnecessary. New support for this view comes from a study of 300 subjects enrolled in a goal-directed resuscitation trial in three urban EDs. The mortality rate was not reduced by ScvO2 monitoring compared with using lactate clearance (hospital mortality 23% vs 17%; P value not signifi cant). SchmidtGAChest 2010;138; 480-483
Using CVP to guide volume resuscitationfailsto acknowledgethatthisparameteris no betterthan a cointoss in predictingwhowillrespondtofluids. Forexample, in a seriesof 150 fluidbolusesgiven topatientswithsepsis in an ICU, a CVP , 8 mm Hg had a positive predictivevalueofonly 47%. 1 Dynamic physiologicparameterssuchaspulsepressurevariation,brachialarterypeakflowvelocityvariation, inferior vena cava collapsibility, and even passive leg raisingare muchsuperiortostaticpredictorssuchas CVP. SchmidtGAChest 2010;138; 480-483
Ecografia della vena cava inferiore VCS VCI v.c.s. Indice di collassabilità: (diametro massimo – diametro minimo / diametro massimo) x 100
Pressione atriale destra Valutazione escursione respiratoria vena cava inferiore
Ecografia polmonare per sindrome alveolo interstiziale bilaterale
Assiomi • La crescita della competenza in ecografia clinica è un nuovo strumento di lavoro dalle grandi potenzialità e non invasivo • E’ possibile gestire le prime fasi di una sepsi grave senza il CVC (ma con l’ecografo e i lattati)
PROTOCOLLO NON INVASIVO • END POINTS: • IC-VCI 50%-30% • PAM > 65mmHg • Cl lat a 6h > 10% • Diuresi > 0,5ml/Kg/h
POPOLAZIONE IN STUDIO SEPSI SEVERA • CRITERI DI ESCLUSIONE: • Stato agonico all’arrivo • Infarto miocardico acuto • Edema polmonare acuto • Arresto cardiorespiratorio • Gravidanza • Indicazione chirurgica nelle prime 3 ore dall’arrivo SHOCKSETTICO CRITERI DI ARRUOLAMENTO: • Età > 18 anni • Criteri diagnostici di sepsi • Segni di ipoperfusione (lattati all’ingresso > 4 mmol/l) e/o PAM < 65 mmHg persistente dopo 500 ml di colloidi o 20ml/kg di cristalloidi in bolo rapido (30min)
RISULTATI (1) CARATTERISTICHE DEL CAMPIONE • 27 pazienti (Febbraio – Agosto 2010): • 11 (41,7%) donne e 16 (59,3%) uomini • età media: 74,6 ± 13,8 anni • 7 pazienti (25,9%) arruolati per criterio di lattati (sepsi severa) e 20 (74,1%) per criterio pressorio (shock settico) RAGGIUNGIMENTO END POINTS ALLA SESTA ORA • IC-VCI ≤50%: 16 pazienti (59,3%) • PAM ≥ 65mmHg: 22 pazienti (81,5%) • CL lac > 10%: 20 pazienti (74,1%) • Diuresi > 0,5ml/kg/h: 22 pazienti (81,5%)
RISULTATI (2) RAGGIUNGIMENTO COMBINATO DEGLI END POINTS • IC-VCI + PAM: 16 pazienti (59,3%) • IC-VCI + PAM + CL lac: 11 pazienti (40,7%) • IC-VCI + PAM + CL lac + diuresi: 9 pazienti (33,3%) • LIQUIDI INFUSI • 4120 ± 1473 ml (vs 4981 ± 2984 ml - studio Rivers) • SWITCH A TERAPIA INVASIVA • Posizionamento CVC in 12 pazienti (44,4%)
RISULTATI (4) *16 pazienti hanno raggiunto il target di IC-VCI entro la sesta ora. In 1 paziente la collassabilità era già bassa all’ingresso. 8 pazienti non hanno mai raggiunto il target. In 2 la VCI non era visualizzabile
CONCLUSIONI • L’ecografia selettiva di VCI e polmone si è rivelata un utile strumento per il monitoraggio del riempimento volemico, permettendo un’infusione di liquidi più adeguata e vicina agli standard internazionali • Lo switch a terapia invasiva è stato necessario in meno della metà dei pazienti • La mortalità intraospedaliera sembra non discostarsi dalla media del gold standard di riferimento. • Nonostante vi sia un trend nel senso di minore mortalità nei pazienti con buona clearance dei lattati (>10% a 6h) e con IC-VCI <50%, la relativa esiguità del campione non consente di confermare statisticamente l’utilità prognostica di questo dato. • I risultati incoraggiano l’organizzazione di uno studio multicentrico di più ampie dimensioni
ESTABLISHED IN 1812 JANUARY 27, 2012 VOL 366 NO.2 Non-invasive EGDT: an easy approach to severe sepsis widely and successfully employed in the Italian Emergency Departments SSSS - SIMEU Simple Sepsis Study