Download
1 / 1
30 likes | 202 Views
Cohort Analysis Of Stillbirth In A Tertiary Hospital In Malaysia Shazni Izana Shahruddin MD(UNIMAS) , Jamiyah Hassan MBBS(UM) MMed (O&G) Department of Obstetrics and Gynecology, Faculty of Medicine, University Malaya.

E N D
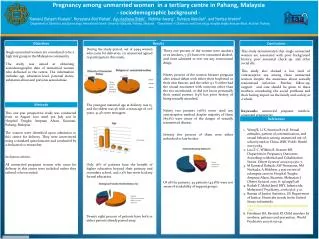
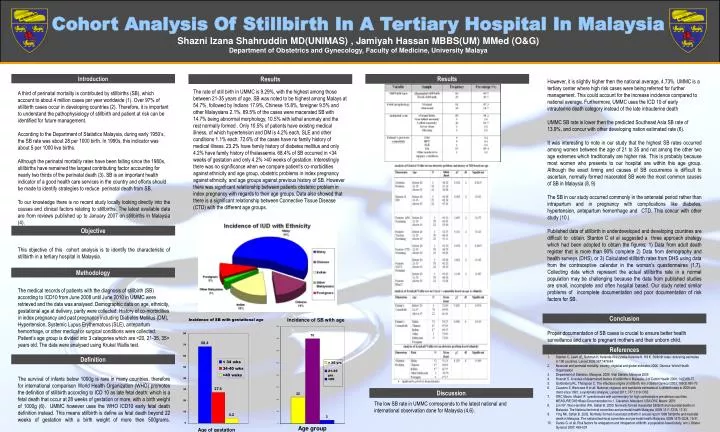
Cohort Analysis Of Stillbirth In A Tertiary Hospital In Malaysia Shazni Izana Shahruddin MD(UNIMAS) , Jamiyah Hassan MBBS(UM) MMed (O&G) Department of Obstetrics and Gynecology, Faculty of Medicine, University Malaya However, it is slightly higher then the national average, 4.73%. UMMC is a tertiary center where high risk cases were being referred for further management. This could account for the increase incidence compared to national average. Furthermore, UMMC uses the ICD 10 of early intrauterine death category instead of the late intrauterine death UMMC SB rate is lower then the predicted Southeast Asia SB rate of 13.9%, and concur with other developing nation estimated rate (6). It was interesting to note in our study that the highest SB rates occurred among women between the age of 21 to 35 and not among the other two age extremes which traditionally are higher risk. This is probably because most women who presents to our hospital are within this age group. Although the exact timing and causes of SB occurrence is difficult to ascertain, normally formed macerated SB were the most common causes of SB in Malaysia (8, 9) The SB in our study occurred commonly in the antenatal period rather than intrapartum and in pregnancy with complications like diabetes, hypertension, antepartum hemorrhage and CTD. This concur with other study (10.) Published data of stillbirth in underdeveloped and developing countries are difficult to obtain. Stanton C et al suggested a three approach strategy which had been adopted to obtain the figures; 1) Data from adult death register that is more than 90% complete 2) Data from demography and health surveys (DHS), or 3) Calculated stillbirth rates from DHS using data from the contraceptive calendar in the woman’s questionnaires (1,7). Collecting data which represent the actual stillbirths rate in a normal population may be challenging because the data from published studies are small, incomplete and often hospital based. Our study noted similar problems of incomplete documentation and poor documentation of risk factors for SB. Proper documentation of SB cases is crucial to ensure better health surveillance and care to pregnant mothers and their unborn child. Introduction Results Results The rate of still birth in UMMC is 9.29%, with the highest among those between 21-35 years of age. SB was noted to be highest among Malays at 54.7%, followed by Indians 17.9%, Chinese 15.8%, foreigner 9.5% and other Malaysians 2.1%. 69.5% of the cases were macerated SB with 14.7% being abnormal morphology, 10.5% with lethal anomaly and the rest normally formed . Only 10.5% of patients have existing medical illness, of which hypertension and DM is 4.2% each, SLE and other conditions 1.1% each. 72.6% of the cases have no family history of medical illness. 23.2% have family history of diabetes mellitus and only 4.2% have family history of thalassemia. 68.4% of SB occurred in <34 weeks of gestation and only 4.2% >40 weeks of gestation. Interestingly there was no significance when we compare patient’s co-morbidities against ethnicity and age group, obstetric problems in index pregnancy against ethnicity, and age groups against previous history of SB. However there was significant relationship between patients obstetric problem in index pregnancy with regards to their age groups. Data also showed that there is a significant relationship between Connective Tissue Disease (CTD) with the different age groups. A third of perinatal mortality is contributed by stillbirths (SB), which account to about 4 million cases per year worldwide (1). Over 97% of stillbirth cases occur in developing countries (2). Therefore, it is important to understand the pathophysiology of stillbirth and patient at risk can be identified for future management. According to the Department of Statistics Malaysia, during early 1950’s, the SB rate was about 28 per 1000 birth. In 1990s, this indicator was about 5 per 1000 live births. Although the perinatal mortality rates have been falling since the 1980s, stillbirths have remained the largest contributing factor accounting for nearly two thirds of the perinatal death (3). SB is an important health indicator of a good health care services in the country and efforts should be made to identify strategies to reduce perinatal death from SB. To our knowledge there is no recent study locally looking directly into the causes and clinical factors relating to stillbirths. The latest available data are from reviews published up to January 2007 on stillbirths in Malaysia (4). This objective of this cohort analysis is to identify the characteristic of stillbirth in a tertiary hospital in Malaysia. The medical records of patients with the diagnosis of stillbirth (SB) according to ICD10 from June 2008 until June 2010 in UMMC were retrieved and the data was analysed. Demographic data on age, ethnicity, gestational age at delivery, parity were collected. History of co-morbidities in index pregnancy and past pregnancy including Diabetes Mellitus (DM), Hypertension, Systemic Lupus Erythematous (SLE), antepartum hemorrhage, or other medical or surgical conditions were collected. Patient’s age group is divided into 3 categories which are <20, 21-35, 35> years old. The data were analysed using Krukal Wallis test. The survival of infants below 1000g is rare in many countries, therefore for international comparison World Health Organization (WHO) promotes the definition of stillbirth according to ICD 10 as late fetal death: which is a fetal death that occur at 28 weeks of gestation or more, with a birth weight of 1000g (6). UMMC however uses the WHO ICD10 early fetal death definition instead. This means stillbirth is define as fetal death beyond 22 weeks of gestation with a birth weight of more then 500grams. Objective Methodology Conclusion References • Stanton C, Lawn JE, Rahman H, Ketende-Wilczynska-Ketende K, Hill K. Stillbirth rates: delivering estimates in 190 countries. Lancet 2006;367:1478-94 • Neonatal and perinatal mortality: country, regional and global estimates 2006. Geneva: World Health Organisation • Department of Statistics, Malaysia. 2009. Vital Statistic Malaysia 2009 • Rosnah S. A review of determinant factors of stillbirths in Malaysia. J of Comm Health 2008; 14(2):68-77. • Goldenberg RL, Thompson C. The infectious origins of stillbirth. Am J Obstet Gynecol 2003; 189(3):861-73 • Causens S, Blencowe H et all. National, regional, and worldwide estimates of s stillbirth rates in 2009 with trend since 1995: a systematic analysis. Lancet 2011; 377:1319-1330 • ORC Macro. Model “A” questionnaire with commentary for high contraceptive prevalence countries. MEASURE DIIS+Basic Documentation no.1. Calverton, Maryland, USA:ORC Macro: 2001. • Lim NY, Wan Hamilton WH, Safiah B. 2000. Normally formed macerated Stillbirth and neonatal deaths in Malaysia. The National technical committee and perinatal health Malaysia, ISSN 1511-7235, 17-33 • Ying NK, Safiah B. 2002. Normally formed macerated stillbirth in annual report 1998 Stillbirths and neonatal death in Malaysia. The national technical committee and perinatal health Malaysia, ISSN 1675-3224, 19-31. • Darios G. et all. Risk factors for antepartum and intrapartum stillbirth: a population-based study. Am J Obstet Gynecol 2007; 499-507 Definition Discussion The low SB rate in UMMC corresponds to the latest national and international observation done for Malaysia (4,6).