Download
1 / 22
230 likes | 711 Views
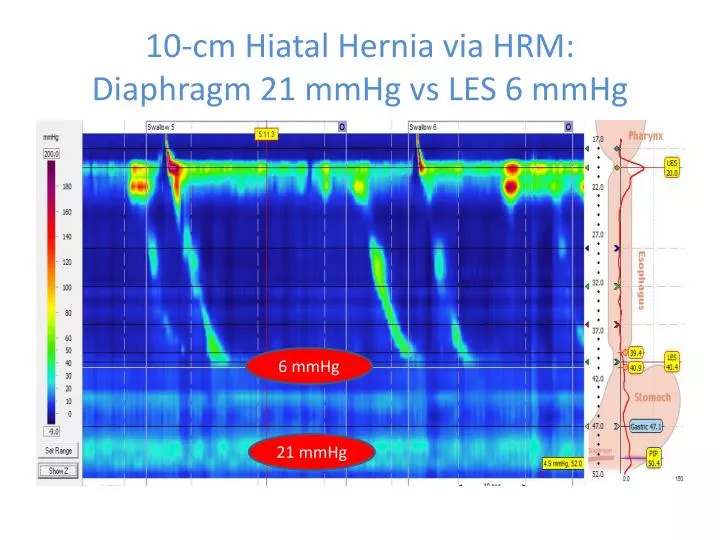
10-cm Hiatal Hernia via HRM: Diaphragm 21 mmHg vs LES 6 mmHg. 6 mmHg. 21 mmHg. 10-cm Hiatal Hernia: Diaphragm (21 mmHg) vs LES (6 mmHg) Pressure Gradient Causes Retrograde Bolus via HRMZ. Demonstrate Real-Time HRM Motility Disorders Using Isobaric Contour & DCI.

E N D
10-cm Hiatal Hernia via HRM:Diaphragm 21 mmHg vs LES 6 mmHg 6 mmHg 21 mmHg
10-cm Hiatal Hernia: Diaphragm (21 mmHg) vs LES (6 mmHg) Pressure Gradient Causes Retrograde Bolus via HRMZ
Demonstrate Real-Time HRM Motility DisordersUsing Isobaric Contour & DCI • Vigorous Achalasia (swallows 4 & 5) • Jackhammer Esophagus (swallow 9) • Post-Fundoplication Obstructive Changes (swallow 3) • Segmental Stair-Step Spasm with Delayed Clearance (swallow 7) • Weak Transition Zone with Retrograde Spasm & Bolus Escape (swallows 3 & 4)
Weak Transition Zone with Spontaneous Retrograde Spasm & Bolus Reflux via HRMZ
Scleroderma Scleroderma is an autoimmune disease of the connective tissue. Scleroderma is characterized by the formation of scar tissue (fibrosis) in the skin and organs of the body. Esophagus disease in scleroderma is characterized by poorly functioning muscle of the lower 2/3 of the esophagus. This can lead to an abnormally wide esophagus, which allows stomach acid to backflow into the esophagus to cause heartburn, inflammation, and potentially scarring. This can eventually lead to difficulty in passing food from the mouth through the esophagus into the stomach. Esohageal manometry confirms the extent of the poor function of the muscles of the scarred lower 2/3 of the esophagus that is common to these patients.
Scleroderma esophagus with peptic stenosis and 3 cm Hiatus Hernia GI Motility online (May 2006) | doi:10.1038/gimo20
Scleroderma via High-Resolution Manometry:No esophageal body peristalsis with Hypotensive LES
What Difference Does HRM Make? My best friend, Eric, lived on 3 PPI’s for 15 years, with terrible reflux that caused him to choke at night. Acid reflux testing revealed massive acid reflux. PPI’s did not stop the physical reflux. However, conventional manometry revealed “normal” esophageal body & LES function. HRM in May 2007 immediately revealed a 3 cm hiatal hernia, with hypotensive LES pressures of only 3 mm Hg, but diaphragmatic pinch pressures during inspiration of 27 mm Hg. So, every time he breathed in, this pressure gradient forced the trapped liquid sitting in his hernia sac to reflux backwards across the weak LES up into his esophagus. Dr. Lee Swanstrom performed a laparoscopic hernia repair with fundoplication, and Eric has lived reflux-free, without PPI’s, for 5 years. When I told him I would use his story as an example today, he asked me to express to you all that, “This has changed my life”. HRM DIRECTLY IMPROVED THE QUALITY OF HIS LIFE!!
24-hour pH-Impedance Testing24-Hour Gastroesophageal Reflux Assessment with combined pH and Impedance (Z) sensors INTUITIVE REFLUX VISUALIZATION The Real-Time Uninterrupted Continuous Assessment of Complete Reflux Activity and Content of 17 cm of the Esophagus Above the Proximal LES
What is impedance, and why add it to pH?Following the Published Path to Diagnose & Treat Esophageal Reflux • Perform wireless capsule 24-hr pH testing to assess the pH level that falls below 4.0 (to diagnose ACID reflux) • As PPI’s merely suppress acid, studies reveal 35% of patients with acid reflux do not improve with PPI’s, but continue to have refluxate >4.0, undetectable with acid-only pH testing • pH-Impedance testing is performed with the patient ON PPI’s • pH < 4.0 is called ACID REFLUX • pH 4.1 - 6.9 is called WEAKLY-ACID REFLUX • pH >7.0 is called NON-ACID REFLUX • Impedance measures the PRESENCE of liquid, gas, or air bolus, and the DIRECTION of its movement • pH sensor simply detects the pH of the retrograde bolus • Software categorizes all three types of reflux for a complete diagnosis that misses nothing!
24-Hour pH-Impedance Catheter Configuration Detects reflux that reaches the proximal esophagus Z channel 17 cm above proximal LES Z channel 15 cm above proximal LES Z channel 9 cm above proximal LES Z channel 7 cm above proximal LES pH channel 5 cm above proximal LES Z channel 5 cm above proximal LES Z channel 3 cm above proximal LES
24-Hour pH & Impedance: Intuitive Color Contour Reveals Bolus Transit Direction & pH Sensor Reveals Acid, Weakly Acid, & Non-Acid Content of the Bolus Z Scale Air Neutral Liquid
Retrograde Weakly-Acid Reflux Episode (pH 5.2) that DOES NOT reach the proximal esophagus , followed by antegrade clearing swallows
Retrograde Acid Reflux Episode (pH 3.1) that DOES reach the proximal esophagus
Retrograde Non-Acid Reflux Episode (pH 7.8) that DOES reach the proximal esophagus Air bolus in proximal esophagus
What Difference Does pH-Impedance Testing Make? • 35% of patients with acid reflux do not fully respond to acid-suppression medication. • pH-impedance testing will accurately determine if these patients have continued non-acid physical reflux that is either weakly or non-acidic reflux. • These patients should have high-resolution impedance manometry to determine if the cause of their reflux is mechanical or obstructive in nature, and if they are a candidate for anti-reflux surgery. • For those whom are surgical candidates, accurate pre-surgical diagnostics have a >95% surgical success with the end of $200/month acid-suppression meds.
Summary • We all entered medicine to provide the most effective medical or surgical interventions for our patient’s illnesses and diseases. • This can only be accomplished with the most accurate and complete diagnostic information available to us. Our treatment is only as good as our assessment of the problem. • At this time, the combination of clinically-validated high-resolution impedance manometry and pH-impedance testing offer the most accurate and complete esophageal functional diagnostics available to assess and treat our dysphagia patients.